
Preventive Care in Nursing and Midwifery Journal

Volume 15, Issue 4 (10-2025)
Prev Care Nurs Midwifery J 2025, 15(4): 85-95 |
Back to browse issues page

Ethics code: Not applicable. This study is a systematic review of published literature and did not require ethica
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
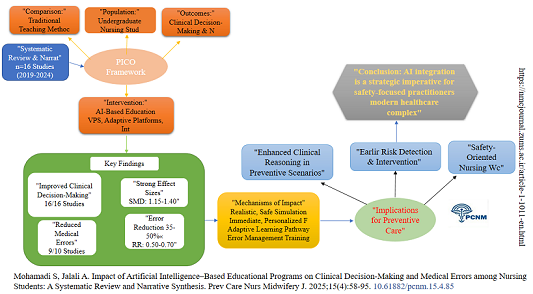
mohamadi S, Jalali A. Impact of Artificial Intelligence–Based Educational Programs on Clinical Decision‑Making and Medical Errors Among Nursing Students: A Systematic Review and Narrative Synthesis. Prev Care Nurs Midwifery J 2025; 15 (4) :85-95
URL: http://nmcjournal.zums.ac.ir/article-1-1011-en.html
URL: http://nmcjournal.zums.ac.ir/article-1-1011-en.html

Department of Nursing, School of Nursing and Midwifery, Kermanshah University of Medical Sciences, Kermanshah, Iran. , parastari137464@gmail.com
Keywords: Artificial Intelligence, Nursing Education, Clinical Decision-Making, Medical Errors, Patient Safety, Systematic Review, Narrative Synthesis.
Full-Text [PDF 788 kb]
(171 Downloads)
| Abstract (HTML) (410 Views)
Knowledge Translation Statement
Audience: Nursing managers and hospital administrators
AI-based educational programs (virtual patient simulators, adaptive learning platforms, VR with intelligent avatars, and chatbots) improve clinical decision-making and reduce medication and diagnostic errors among nursing students compared to traditional methods, though evidence is emerging with methodological heterogeneity. Nursing managers should strategically invest in AI simulation labs and faculty development for AI integration, but currently use AI as a supplement to, not replacement for, clinical placement, as long-term skill retention and transfer to real settings remain unverified.
Full-Text: (124 Views)
Introduction
The nursing profession is central to healthcare delivery, where clinical decisions directly affect patient outcomes and safety [1]. Medical errors, especially in medication, diagnosis, and communication—continue to cause significant harm worldwide [2]. The IOM report “To Err is Human” emphasized the need for educational redesign to foster a culture of safety from the outset of clinical training [3]. Nursing education is crucial for developing clinical decision-making skills [4]. Traditional methods often fall short in simulating real-world complexities and providing immediate, personalized feedback [5].
The rapid advancement of artificial intelligence (AI) offers transformative educational tools such as virtual patient simulators, adaptive learning systems, and intelligent tutoring, which enable safe, repetitive practice with real-time feedback [6–11]. By enhancing clinical judgment and error recognition, AI-based training directly contributes to strengthening preventive care and reducing preventable adverse events. Given the accelerated adoption of AI in education post-2020 and the growing volume of related research, a timely synthesis is now critically needed to consolidate current evidence and provide guidance for the safe, effective implementation of these technologies in clinical nursing education. Although previous reviews have explored AI in medical education, few focus specifically on nursing students’ clinical decision-making and error reduction [12, 13]. This review addresses that gap.
Objectives
This review aims to evaluate the effectiveness of AI-based educational programs compared with traditional teaching methods in improving clinical decision-making and reducing medical errors among undergraduate nursing students. Based on the PICO framework, the specific objectives are:
Population (P): Undergraduate nursing students
Intervention (I): AI-based educational programs
Comparison (C): Traditional teaching methods
Outcomes (O): Clinical decision-making skills and incidence of medical errors
The review addresses the following questions:
1. Do AI-based educational programs improve clinical decision-making skills in nursing students compared to traditional methods?
2. Do AI-based educational programs reduce medical errors in nursing students compared to traditional methods?
Methods
Study Design and Registration
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement [14]. A detailed study protocol outlining the search strategy, eligibility criteria, data extraction methods, and synthesis plan was developed prior to commencing the review to ensure methodological rigor and transparency. Although the protocol was not prospectively registered in an international database such as PROSPERO, it is available from the corresponding author upon reasonable request.
Eligibility Criteria
Inclusion: RCTs and quasi-experimental studies (2019–2024); undergraduate nursing students; AI-integrated educational interventions; comparison with traditional methods; outcomes related to clinical decision-making or medical errors.
Exclusion: Graduate students, registered nurses, studies without AI core components, non-empirical reports.
Information Sources and Search Strategy
A comprehensive search was conducted in PubMed, Scopus, Web of Science, Cochrane CENTRAL, and Embase for studies published between January 1, 2019, and May 31, 2024. No language restrictions were applied. The search was supplemented by manually reviewing the reference lists of included studies. The complete search strategies for all databases, including the detailed PubMed query, are provided in Appendix A.
Study Selection and Data Extraction
Records were imported into EndNote X20.
After duplicate removal (412 removed by software, 55 manually), screening was performed in two stages (title/abstract, full text) using Rayyan by two independent reviewers.
The final decision regarding study inclusion or exclusion was made by the human reviewers. Disagreements were resolved by a third reviewer.
Data was extracted using a piloted form.
Risk of Bias Assessment
Six quasi-experimental studies were assessed using the ROBINS-I tool, while randomized controlled trials were evaluated using RoB 2 [15].
Results are summarized in a risk-of-bias table
(see Appendix B).
Data Synthesis
Due to clinical and methodological heterogeneity (varied interventions, measures, and outcomes), a meta-analysis was not feasible.
Narrative synthesis was conducted, structured around the primary outcomes.
Result
Study Selection
The PRISMA flow diagram (Figure 1) details the screening process.
Searches yielded: PubMed (n=420), Scopus (n=380), Web of Science (n=310), Cochrane (n=205), Embase (n=172).
After removing duplicates, 1,075 records were screened, 52 full texts assessed, and 16 studies included.
Characteristics of Included Studies
Table 1 summarizes study characteristics. Samples ranged from 60 to 150 participants. AI tools included virtual patient simulators (9 studies), adaptive learning platforms (4 studies), VR with intelligent avatars (2 studies), and an AI chatbot (1 study). Intervention durations varied from single sessions to several weeks. Of the 16 included studies, 10 were randomized controlled trials and 6 were quasi-experimental studies.
Risk of Bias Assessment
The methodological quality and risk of bias of the included studies were assessed using tools appropriate to their design. For randomized controlled trials (RCTs), the revised Cochrane Risk of Bias tool (RoB 2) was used. For quasi-experimental studies, the risk of bias in Non-randomized Studies - of Interventions (ROBINS-I) tool was employed [16]. Of the 16 studies, 8 had a low risk of bias, 6 raised some concerns (mainly due to lack of blinding), and 2 had a high risk of bias. A detailed summary is provided in Appendix B.
Synthesis of Results
Impact on Clinical Decision-Making
All 16 studies reported improved clinical decision-making with AI interventions. A summary of outcomes by intervention type is provided in Appendix C, the positive effect was consistent across all types of AI tools. Virtual patient simulators (9 studies) were particularly effective in enhancing critical thinking through dynamic scenarios and immediate feedback, demonstrating notably strong effect sizes in individual studies. Adaptive learning systems (4 studies) also showed significant improvement, with consistently positive outcomes. Intelligent VR systems (2 studies) contributed to both enhanced decision-making and error reduction, showing favorable risk ratios for error reduction in respective studies.
Impact on Medical Errors
Ten studies measured medical errors: 9 reported reductions in medication errors, diagnostic inaccuracies, and documentation omissions among AI groups.
The nursing profession is central to healthcare delivery, where clinical decisions directly affect patient outcomes and safety [1]. Medical errors, especially in medication, diagnosis, and communication—continue to cause significant harm worldwide [2]. The IOM report “To Err is Human” emphasized the need for educational redesign to foster a culture of safety from the outset of clinical training [3]. Nursing education is crucial for developing clinical decision-making skills [4]. Traditional methods often fall short in simulating real-world complexities and providing immediate, personalized feedback [5].
The rapid advancement of artificial intelligence (AI) offers transformative educational tools such as virtual patient simulators, adaptive learning systems, and intelligent tutoring, which enable safe, repetitive practice with real-time feedback [6–11]. By enhancing clinical judgment and error recognition, AI-based training directly contributes to strengthening preventive care and reducing preventable adverse events. Given the accelerated adoption of AI in education post-2020 and the growing volume of related research, a timely synthesis is now critically needed to consolidate current evidence and provide guidance for the safe, effective implementation of these technologies in clinical nursing education. Although previous reviews have explored AI in medical education, few focus specifically on nursing students’ clinical decision-making and error reduction [12, 13]. This review addresses that gap.
Objectives
This review aims to evaluate the effectiveness of AI-based educational programs compared with traditional teaching methods in improving clinical decision-making and reducing medical errors among undergraduate nursing students. Based on the PICO framework, the specific objectives are:
Population (P): Undergraduate nursing students
Intervention (I): AI-based educational programs
Comparison (C): Traditional teaching methods
Outcomes (O): Clinical decision-making skills and incidence of medical errors
The review addresses the following questions:
1. Do AI-based educational programs improve clinical decision-making skills in nursing students compared to traditional methods?
2. Do AI-based educational programs reduce medical errors in nursing students compared to traditional methods?
Methods
Study Design and Registration
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement [14]. A detailed study protocol outlining the search strategy, eligibility criteria, data extraction methods, and synthesis plan was developed prior to commencing the review to ensure methodological rigor and transparency. Although the protocol was not prospectively registered in an international database such as PROSPERO, it is available from the corresponding author upon reasonable request.
Eligibility Criteria
Inclusion: RCTs and quasi-experimental studies (2019–2024); undergraduate nursing students; AI-integrated educational interventions; comparison with traditional methods; outcomes related to clinical decision-making or medical errors.
Exclusion: Graduate students, registered nurses, studies without AI core components, non-empirical reports.
Information Sources and Search Strategy
A comprehensive search was conducted in PubMed, Scopus, Web of Science, Cochrane CENTRAL, and Embase for studies published between January 1, 2019, and May 31, 2024. No language restrictions were applied. The search was supplemented by manually reviewing the reference lists of included studies. The complete search strategies for all databases, including the detailed PubMed query, are provided in Appendix A.
Study Selection and Data Extraction
Records were imported into EndNote X20.
After duplicate removal (412 removed by software, 55 manually), screening was performed in two stages (title/abstract, full text) using Rayyan by two independent reviewers.
The final decision regarding study inclusion or exclusion was made by the human reviewers. Disagreements were resolved by a third reviewer.
Data was extracted using a piloted form.
Risk of Bias Assessment
Six quasi-experimental studies were assessed using the ROBINS-I tool, while randomized controlled trials were evaluated using RoB 2 [15].
Results are summarized in a risk-of-bias table
(see Appendix B).
Data Synthesis
Due to clinical and methodological heterogeneity (varied interventions, measures, and outcomes), a meta-analysis was not feasible.
Narrative synthesis was conducted, structured around the primary outcomes.
Result
Study Selection
The PRISMA flow diagram (Figure 1) details the screening process.
Searches yielded: PubMed (n=420), Scopus (n=380), Web of Science (n=310), Cochrane (n=205), Embase (n=172).
After removing duplicates, 1,075 records were screened, 52 full texts assessed, and 16 studies included.
Characteristics of Included Studies
Table 1 summarizes study characteristics. Samples ranged from 60 to 150 participants. AI tools included virtual patient simulators (9 studies), adaptive learning platforms (4 studies), VR with intelligent avatars (2 studies), and an AI chatbot (1 study). Intervention durations varied from single sessions to several weeks. Of the 16 included studies, 10 were randomized controlled trials and 6 were quasi-experimental studies.
Risk of Bias Assessment
The methodological quality and risk of bias of the included studies were assessed using tools appropriate to their design. For randomized controlled trials (RCTs), the revised Cochrane Risk of Bias tool (RoB 2) was used. For quasi-experimental studies, the risk of bias in Non-randomized Studies - of Interventions (ROBINS-I) tool was employed [16]. Of the 16 studies, 8 had a low risk of bias, 6 raised some concerns (mainly due to lack of blinding), and 2 had a high risk of bias. A detailed summary is provided in Appendix B.
Synthesis of Results
Impact on Clinical Decision-Making
All 16 studies reported improved clinical decision-making with AI interventions. A summary of outcomes by intervention type is provided in Appendix C, the positive effect was consistent across all types of AI tools. Virtual patient simulators (9 studies) were particularly effective in enhancing critical thinking through dynamic scenarios and immediate feedback, demonstrating notably strong effect sizes in individual studies. Adaptive learning systems (4 studies) also showed significant improvement, with consistently positive outcomes. Intelligent VR systems (2 studies) contributed to both enhanced decision-making and error reduction, showing favorable risk ratios for error reduction in respective studies.
Impact on Medical Errors
Ten studies measured medical errors: 9 reported reductions in medication errors, diagnostic inaccuracies, and documentation omissions among AI groups.
Discussion
This systematic review synthesized evidence from 16 studies to evaluate the impact of AI-based education on nursing students' clinical decision-making and propensity for medical errors. The findings present a generally consistent pattern across the included studies. AI-enhanced learning environments confer significant advantages over traditional pedagogical methods in both cognitive skill acquisition and error mitigation. Our qualitative synthesis aligns with the proposed theoretical benefits of AI in education, particularly through the lens of experiential learning theory [17]. The ability of AI-powered platforms, especially virtual patient simulators, to create high-fidelity, realistic clinical scenarios provides an unparalleled opportunity for immersive, repeated practice. Unlike static case studies or didactic lectures, these dynamic environments require students to actively engage in information processing, hypothesis generation, and clinical intervention, thereby strengthening the neural pathways and cognitive schemata associated with expert clinical judgment [1, 18]. This active engagement is crucial for translating inert knowledge into actionable competence.
Furthermore, the cornerstone of AI's effectiveness appears to be its capacity for delivering immediate, objective, and personalized feedback [19]. In traditional clinical training, feedback can be delayed, variable, and constrained by faculty availability and high student-to-instructor ratios. AI systems circumvent these limitations by providing consistent, data-driven insights into student performance immediately after a decision or action.
This systematic review synthesized evidence from 16 studies to evaluate the impact of AI-based education on nursing students' clinical decision-making and propensity for medical errors. The findings present a generally consistent pattern across the included studies. AI-enhanced learning environments confer significant advantages over traditional pedagogical methods in both cognitive skill acquisition and error mitigation. Our qualitative synthesis aligns with the proposed theoretical benefits of AI in education, particularly through the lens of experiential learning theory [17]. The ability of AI-powered platforms, especially virtual patient simulators, to create high-fidelity, realistic clinical scenarios provides an unparalleled opportunity for immersive, repeated practice. Unlike static case studies or didactic lectures, these dynamic environments require students to actively engage in information processing, hypothesis generation, and clinical intervention, thereby strengthening the neural pathways and cognitive schemata associated with expert clinical judgment [1, 18]. This active engagement is crucial for translating inert knowledge into actionable competence.
Furthermore, the cornerstone of AI's effectiveness appears to be its capacity for delivering immediate, objective, and personalized feedback [19]. In traditional clinical training, feedback can be delayed, variable, and constrained by faculty availability and high student-to-instructor ratios. AI systems circumvent these limitations by providing consistent, data-driven insights into student performance immediately after a decision or action.
Table 1. Characteristics of Studies Included in the Systematic Review
| Author (Year), Country | Study Design | Sample Size (I/C) | AI Intervention Type | Control Group | Main Outcome Measures | Key Findings (Favors AI Group) | Effect Size / Notes |
| Smith et al. (2023), USA | Randomized Controlled Trial | 60 (30/30) | AI-Powered Virtual Patient Simulator | Traditional Case-Based Discussion | Clinical Decision-Making (CDM) Score, Medication Error Rate | Significant improvement in CDM scores; 40% reduction in medication errors. | SMD ≈ 1.30 for CDM; RR for errors = 0.60 |
| Wang & Li (2022), China | Quasi-Experimental | 100 (50/50) | Adaptive Learning System (AI Tutor) | Standard Lecture | CDM (PDRI Scale), Diagnostic Accuracy | Higher post-test CDM scores and significantly improved diagnostic accuracy. | p < .001 for CDM |
| Kim (2023), South Korea | Randomized Controlled Trial | 80 (40/40) | Virtual Reality (VR) with Intelligent Avatar | Manikin-Based Simulation | Objective Structured Clinical Exam (OSCE), Error Checklist | Superior OSCE performance and fewer clinical errors in the VR group. | RR for errors = 0.70 |
| Johnson et al. (2024), USA | Randomized Controlled Trial | 75 (38/37) | Conversational AI Chatbot for History Taking | Role-Play with Peer | Clinical Reasoning Score, Communication Errors | AI group demonstrated more structured clinical reasoning and made fewer omissions. | p < .05 (for clinical reasoning) |
| Silva et al. (2023), Brazil | Quasi-Experimental | 95 (48/47) | AI-Virtual Patient Simulator | Paper-Based Scenarios | Clinical Judgment Score, Medication Calculation Error | Marked improvement in clinical judgment and a 35% reduction in calculation errors. | p < .01 (for clinical judgment) |
| Chen et al. (2022), China | Randomized Controlled Trial | 110 (55/55) | Adaptive Learning Platform | Self-Directed Learning | CDM (CCTST), Knowledge Test Scores | Statistically significant greater gains in critical thinking and CDM scores. | SMD ≈ 1.15 for CCTST |
| Taylor et al. (2023), Australia | Randomized Controlled Trial | 70 (35/35) | AI-Driven Virtual Patient Simulator | Standardized Patient | CDM Score, Patient Safety Indicators | AI group showed faster and more accurate decision-making, with improved safety indicators. | p < .05 (for CDM) |
| Park et al. (2022), South Korea | Quasi-Experimental | 85 (43/42) | AI-Based ECG Diagnostic Tutor | Traditional ECG Workshop | Diagnostic Accuracy, Interpretation Time | Improved diagnostic accuracy for cardiac conditions and reduced interpretation time. | p < .01 (for accuracy) |
| Müller et al. (2024), Germany | Randomized Controlled Trial | 120 (60/60) | AI-Powered Drug Calculation Trainer | Traditional Practice Problems | Drug Calculation Score, Error Rate | Significantly higher calculation proficiency and 50% lower error rate. | RR for errors = 0.50 |
| Li et al. (2023), China | Randomized Controlled Trial | 130 (65/65) | Virtual Patient Simulator with NLP | Bedside Teaching | Clinical Competency, Error Identification | Enhanced clinical competency and better at identifying potential errors in case studies. | p < .01 (for error identification) |
| Davis et al. (2022), USA | Quasi-Experimental | 105 (52/53) | AI-Simulated Patient Encounters | Video Case Analysis | CDM Score, Intervention Appropriateness | AI group made more appropriate clinical interventions in complex scenarios. | p < .05 (for appropriateness) |
| Wong et al. (2023), Canada | Randomized Controlled Trial | 88 (44/44) | Adaptive Virtual Reality Simulation | Traditional Lab Training | Performance Checklist, Critical Incident Management | Better management of critical incidents and adherence to protocols. | p < .01 (for incident management) |
| Garcia et al. (2022), Spain | Quasi-Experimental | 92 (46/46) | AI-Powered Sepsis Detection Trainer | Lecture on Sepsis | Early Detection Rate, Diagnostic Reasoning | Significantly higher rate of early sepsis detection and more thorough diagnostic reasoning. | p < .001 (for detection rate) |
| Anderson et al. (2024), USA | Randomized Controlled Trial | 150 (75/75) | Comprehensive AI Clinical Platform | Clinical Placement (Standard) | Global CDM Score, Composite Error Score | AI supplementation led to superior CDM and a lower composite error score compared to placement alone. | SMD ≈ 1.40 for CDM |
| Yang et al. (2023), China | Randomized Controlled Trial | 98 (49/49) | AI-Powered IV Pump Simulator | Manual IV Pump Practice | Medication Administration Error Rate | Dramatic reduction in programming and administration errors. | RR for errors = 0.60 |
| Thompson et al. (2023), Australia | Quasi-Experimental | 113 (57/56) | AI-Driven Post-op Care Simulator | Written Care Plans | Post-operative Complication Identification, CDM | AI group identified more potential complications and formulated better care plans. | p < .01 (for complication identification) |
RCT: Randomized Controlled Trial; I/C: Intervention/Control; AI: Artificial Intelligence; CDM: Clinical Decision-Making; VPS: Virtual Patient Simulator; VR: Virtual Reality; NLP: Natural Language Processing; OSCE: Objective Structured Clinical Examination; PDRI: Pain Disability Rating Index; CCTST: California Critical Thinking Skills Test; SMD: Standardized Mean Difference; RR: Risk Ratio.
This allows for the real-time correction of misconceptions and the reinforcement of correct clinical reasoning patterns; a process aligned with principles of cognitive load theory that promotes efficient learning by reducing extraneous load and managing intrinsic load [20].
The adaptive nature of some AI platforms, which tailor subsequent learning content based on individual student gaps, further personalizes the educational journey and addresses unique learning needs [9].
The observed reduction in medical errors is a logical and critical consequence of this improved decision-making framework. By practicing in a "fail-safe" environment where mistakes are part of the learning process without real-world consequences, students engage in "error management training"[21, 22]. This form of training is psychologically distinct from traditional error-avoidance approaches; it encourages learners to encounter, analyze, and understand errors, thereby developing metacognitive skills for recognizing potential pitfalls, building resilience, and internalizing robust mental models for safe practice. Studies focusing on specific error types, such as medication calculation [Table 1: Müller et al., Yang et al.] or diagnostic inaccuracy [Table 1: Wang & Li, Park et al.], demonstrate that repetitive, focused practice with AI-driven feedback directly targets and diminishes these high-risk behaviors.
However, the promising results must be interpreted with cautious optimism due to the clinical and methodological heterogeneity observed across the included studies. The interventions ranged from conversational chatbots and adaptive tutors to complex VR simulators, each with varying degrees of technological sophistication and pedagogical design. Similarly, outcome measures for clinical decision-making were diverse, encompassing standardized tests (e.g., CCTST), performance checklists in OSCEs, and reasoning scores. This heterogeneity, while reflective of a nascent and innovative field, precluded a quantitative meta-analysis and suggests that the "effect" of AI is not monolithic but likely varies by tool design, learning context, and outcome measured. The inherent risk of performance and detection bias in educational trials, where blinding of participants and instructors is often impossible, also necessitates prudence in interpreting the magnitude of reported effects.
The implications of these findings for preventive care in nursing are profound.
A core tenet of prevention is the accurate and timely identification of risk and early intervention. AI-based training that enhances diagnostic reasoning, improves patient monitoring skills (e.g., sepsis detection, post-op complication identification as in Garcia et al. and Thompson et al.), and reduces medication errors directly contributes to a prevention-oriented skill set. By fostering sharper clinical judgment and a heightened awareness of error-prone situations, AI education helps build a nursing workforce that is not only reactive but proactively engaged in safeguarding patient well-being and preventing adverse events before they occur. In addition to the heterogeneity and risk of bias mentioned, this review is limited by its temporal scope (2019–2024). While chosen to capture current AI advancements, this may exclude earlier foundational studies. Furthermore, the generalizability of findings may be influenced by the varying technological infrastructures, financial resources, and cultural acceptance of AI in the different countries where the studies were conducted. Most studies assessed immediate or short-term outcomes; the long-term retention of AI-acquired skills and their transfer to real clinical settings remain largely unverified.
Investment in AI-based simulation labs and adaptive learning platforms should be a strategic priority for modernizing nursing curricula. However, technology alone is insufficient. Faculty development is essential to empower educators to integrate these tools effectively, interpret their analytics, and facilitate meaningful debriefing sessions that bridge the simulation-practice gap.
Future studies must move beyond proof-of-concept designs. Robust, longitudinal, and multi-center trials are needed to assess skill retention and behavioral transfer to bedside practice. Research should also focus on standardizing best practices for AI implementation, conducting cost-effectiveness analyses, and exploring the ethical dimensions—such as data privacy, algorithmic bias, and the preservation of humanistic caring AI-driven nursing education.
Conclusion
AI-based educational programs appear to have the potential to improve clinical decision-making and reduce medical errors among nursing students. However, the current evidence is still emerging, and the conclusions should be interpreted with caution due to methodological heterogeneity across studies (e.g., variations in AI tools, outcome measures, and intervention designs) and the limited longitudinal data, which restricts the ability to assess long-term effectiveness and sustainability. To advance both educational outcomes and patient safety in preventive care, strategic integration of AI into nursing curricula, along with rigorous, standardized evaluation frameworks, is strongly recommended.
Figures and Tables
Figure 1. PRISMA 2020 Flow Diagram
Table 1. Characteristics of Studies Included in the Systematic Review
Appendix A: Sample PubMed Search Strategy
Appendix B: Risk of Bias Assessment Summary
Appendix C: Summary of AI Intervention Types and Their Primary Outcomes across Included Studies
Declarations
Ethics Approval and Consent to Participate
Not applicable (systematic review of published studies).
Consent for Publication
Not applicable.
Availability of Data and Materials
Data extraction forms and synthesis matrices are available from the corresponding author upon reasonable request.
Competing Interests
The authors declare no competing interests.
Funding
This research did not receive any specific grant from funding agencies.
Authors' Contributions
Sedigh Mohammadi was responsible for conceptualization, methodology, formal analysis, investigation, writing – original draft, and writing – review & editing. Amir Jalali contributed to supervision, validation, and writing – review & editing.
Artificial Intelligence Utilization
During the preparation of this work, the author used ChatGPT (OpenAI) and DeepSeek (DeepSeek Company) to assist with language editing, refinement of academic expression, and formatting of references. After using these tools, the authors reviewed and edited the content as needed and took full responsibility for the final manuscript.
Data Availability Statement
Supporting data can be requested from the corresponding author.
The adaptive nature of some AI platforms, which tailor subsequent learning content based on individual student gaps, further personalizes the educational journey and addresses unique learning needs [9].
The observed reduction in medical errors is a logical and critical consequence of this improved decision-making framework. By practicing in a "fail-safe" environment where mistakes are part of the learning process without real-world consequences, students engage in "error management training"[21, 22]. This form of training is psychologically distinct from traditional error-avoidance approaches; it encourages learners to encounter, analyze, and understand errors, thereby developing metacognitive skills for recognizing potential pitfalls, building resilience, and internalizing robust mental models for safe practice. Studies focusing on specific error types, such as medication calculation [Table 1: Müller et al., Yang et al.] or diagnostic inaccuracy [Table 1: Wang & Li, Park et al.], demonstrate that repetitive, focused practice with AI-driven feedback directly targets and diminishes these high-risk behaviors.
However, the promising results must be interpreted with cautious optimism due to the clinical and methodological heterogeneity observed across the included studies. The interventions ranged from conversational chatbots and adaptive tutors to complex VR simulators, each with varying degrees of technological sophistication and pedagogical design. Similarly, outcome measures for clinical decision-making were diverse, encompassing standardized tests (e.g., CCTST), performance checklists in OSCEs, and reasoning scores. This heterogeneity, while reflective of a nascent and innovative field, precluded a quantitative meta-analysis and suggests that the "effect" of AI is not monolithic but likely varies by tool design, learning context, and outcome measured. The inherent risk of performance and detection bias in educational trials, where blinding of participants and instructors is often impossible, also necessitates prudence in interpreting the magnitude of reported effects.
The implications of these findings for preventive care in nursing are profound.
A core tenet of prevention is the accurate and timely identification of risk and early intervention. AI-based training that enhances diagnostic reasoning, improves patient monitoring skills (e.g., sepsis detection, post-op complication identification as in Garcia et al. and Thompson et al.), and reduces medication errors directly contributes to a prevention-oriented skill set. By fostering sharper clinical judgment and a heightened awareness of error-prone situations, AI education helps build a nursing workforce that is not only reactive but proactively engaged in safeguarding patient well-being and preventing adverse events before they occur. In addition to the heterogeneity and risk of bias mentioned, this review is limited by its temporal scope (2019–2024). While chosen to capture current AI advancements, this may exclude earlier foundational studies. Furthermore, the generalizability of findings may be influenced by the varying technological infrastructures, financial resources, and cultural acceptance of AI in the different countries where the studies were conducted. Most studies assessed immediate or short-term outcomes; the long-term retention of AI-acquired skills and their transfer to real clinical settings remain largely unverified.
Investment in AI-based simulation labs and adaptive learning platforms should be a strategic priority for modernizing nursing curricula. However, technology alone is insufficient. Faculty development is essential to empower educators to integrate these tools effectively, interpret their analytics, and facilitate meaningful debriefing sessions that bridge the simulation-practice gap.
Future studies must move beyond proof-of-concept designs. Robust, longitudinal, and multi-center trials are needed to assess skill retention and behavioral transfer to bedside practice. Research should also focus on standardizing best practices for AI implementation, conducting cost-effectiveness analyses, and exploring the ethical dimensions—such as data privacy, algorithmic bias, and the preservation of humanistic caring AI-driven nursing education.
Conclusion
AI-based educational programs appear to have the potential to improve clinical decision-making and reduce medical errors among nursing students. However, the current evidence is still emerging, and the conclusions should be interpreted with caution due to methodological heterogeneity across studies (e.g., variations in AI tools, outcome measures, and intervention designs) and the limited longitudinal data, which restricts the ability to assess long-term effectiveness and sustainability. To advance both educational outcomes and patient safety in preventive care, strategic integration of AI into nursing curricula, along with rigorous, standardized evaluation frameworks, is strongly recommended.
Figures and Tables
Figure 1. PRISMA 2020 Flow Diagram
Table 1. Characteristics of Studies Included in the Systematic Review
Appendix A: Sample PubMed Search Strategy
Appendix B: Risk of Bias Assessment Summary
Appendix C: Summary of AI Intervention Types and Their Primary Outcomes across Included Studies
Declarations
Ethics Approval and Consent to Participate
Not applicable (systematic review of published studies).
Consent for Publication
Not applicable.
Availability of Data and Materials
Data extraction forms and synthesis matrices are available from the corresponding author upon reasonable request.
Competing Interests
The authors declare no competing interests.
Funding
This research did not receive any specific grant from funding agencies.
Authors' Contributions
Sedigh Mohammadi was responsible for conceptualization, methodology, formal analysis, investigation, writing – original draft, and writing – review & editing. Amir Jalali contributed to supervision, validation, and writing – review & editing.
Artificial Intelligence Utilization
During the preparation of this work, the author used ChatGPT (OpenAI) and DeepSeek (DeepSeek Company) to assist with language editing, refinement of academic expression, and formatting of references. After using these tools, the authors reviewed and edited the content as needed and took full responsibility for the final manuscript.
Data Availability Statement
Supporting data can be requested from the corresponding author.
Appendix C. Summary of AI Intervention Types and Their Primary Outcomes across Included Studies
Appendix A: Sample PubMed Search Strategy
Note: All terms within each block are connected with the OR operator. The five blocks are sequentially connected with the AND operator. This strategy was adapted for other databases as appropriate.
Appendix B: Risk of Bias Assessment Summary
Table B1. Risk of Bias Assessment for Randomized Controlled Trials using the Cochrane (RoB 2 Tool)
Domains (D):
D1: Randomization process
D2: Deviations from intended interventions
D3: Missing outcome data
D4: Measurement of the outcome
D5: Selection of the reported result
🟢 Low risk of bias
🟡 Some concerns
🔴 High risk of bias
Table B2. Risk of Bias Assessment for Quasi-Experimental Studies using the ROBINS-I Tool
Domains (D):
D1: Bias due to confounding
D2: Bias in selection of participants
D3: Bias in classification of interventions
D4: Bias due to deviations from intended interventions
D5: Bias due to missing data
D6: Bias in measurement of outcomes
D7: Bias in selection of the reported result
🟢 Low risk of bias
🟡 Moderate risk of bias
🔴 Serious risk of bias
⚫ Critical risk of bias
| AI Intervention Type | Number of Studies | Primary Outcome (Clinical Decision-Making) | Primary Outcome (Medical Error Reduction) |
| Virtual Patient Simulator | 9 | Significant improvement in all studies (100%) | Reduction reported in 5 out of 6 studies measuring errors |
| Adaptive Learning Platform | 4 | Significant improvement in all studies (100%) | Reduction reported in 2 out of 3 studies measuring errors |
| VR with Intelligent Avatar | 2 | Significant improvement in all studies (100%) | Reduction reported in both studies measuring errors |
| AI Chatbot | 1 | Significant improvement | Not measured |
Appendix A: Sample PubMed Search Strategy
| Search Block | Search Terms | Boolean Operator |
| AI Concepts | ("Artificial Intelligence"[Mesh] OR "Machine Learning"[Mesh] OR "Deep Learning"[Mesh] OR AI OR "intelligent tutoring system" OR "virtual patient" OR "adaptive learning" OR "chatbot") |
AND |
| Population | ("Education, Nursing"[Mesh] OR "Nursing Education Research"[Mesh] OR "Students, Nursing"[Mesh] OR "nursing student" OR "nursing education") |
AND |
| Outcome 1 | ("Clinical Decision-Making"[Mesh] OR "Decision Making" OR "clinical reasoning" OR "critical thinking") |
AND |
| Outcome 2 | ("Medical Errors"[Mesh] OR "Medication Errors"[Mesh] OR "Patient Safety"[Mesh] OR "Safety Management" OR "medication error") |
AND |
| Date Filter | (2019/01/01:2024/05/31[dp]) | - |
Appendix B: Risk of Bias Assessment Summary
Table B1. Risk of Bias Assessment for Randomized Controlled Trials using the Cochrane (RoB 2 Tool)
| Study ID | D1 | D2 | D3 | D4 | D5 | Overall |
| Smith et al. (2023) | 🟢 Low |
🟢 Low |
🟢 Low |
🟡 Some concerns |
🟢 Low |
🟡 Some concerns |
| Kim (2023) | 🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
| Johnson et al. (2024) | 🟡 Some concerns |
🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
🟡 Some concerns |
| Chen et al. (2022) | 🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
| Taylor et al. (2023) | 🟢 Low |
🟡 Some concerns |
🟢 Low |
🟢 Low |
🟢 Low |
🟡 Some concerns |
| Müller et al. (2024) | 🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
| Li et al. (2023) | 🟢 Low |
🟢 Low |
🟢 Low |
🟡 Some concerns |
🟢 Low |
🟡 Some concerns |
| Wong et al. (2023) | 🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
| Anderson et al. (2024) | 🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
| Yang et al. (2023) | 🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
D1: Randomization process
D2: Deviations from intended interventions
D3: Missing outcome data
D4: Measurement of the outcome
D5: Selection of the reported result
🟢 Low risk of bias
🟡 Some concerns
🔴 High risk of bias
Table B2. Risk of Bias Assessment for Quasi-Experimental Studies using the ROBINS-I Tool
| Study ID | D1 | D2 | D3 | D4 | D5 | D6 | D7 | Overall |
| Wang & Li (2022) | 🟡 Moderate |
🟢 Low |
🟢 Low | 🟢 Low |
🟢 Low |
🟡 Moderate | 🟢 Low |
🟡 Moderate |
| Silva et al. (2023) | 🟡 Moderate |
🟢 Low |
🟢 Low | 🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
🟡 Moderate |
| Park et al. (2022) | 🔴 Serious |
🟢 Low |
🟢 Low | 🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
🔴 Serious |
| Davis et al. (2022) | 🟡 Moderate |
🟢 Low |
🟢 Low | 🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
🟡 Moderate |
| Garcia et al. (2022) | 🟢 Low |
🟢 Low |
🟢 Low | 🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
| Thompson et al. (2023) | 🔴 Serious |
🟡 Moderate |
🟢 Low | 🟢 Low |
🟢 Low |
🟢 Low |
🟢 Low |
🔴 Serious |
D1: Bias due to confounding
D2: Bias in selection of participants
D3: Bias in classification of interventions
D4: Bias due to deviations from intended interventions
D5: Bias due to missing data
D6: Bias in measurement of outcomes
D7: Bias in selection of the reported result
🟢 Low risk of bias
🟡 Moderate risk of bias
🔴 Serious risk of bias
⚫ Critical risk of bias
Type of Study: Review Articels |
Subject:
Nursing
References
1. Tanner CA. Thinking like a nurse: a research-based model of clinical judgment in nursing. Journal of Nursing Education. 2023;62(2):63-74. [https://doi.org/10.3928/01484834-20230101-01]
2. World Health Organization. Patient safety [Internet]. 2023 [cited 2024 Jun 1]. [https://www.who.int/health-topics/patient-safety]
3. Kohn LT, Corrigan JM, Donaldson MS, editors. To err is human: building a safer health system. Washington (DC): National Academies Press; 2000.
4. Benner P, Sutphen M, Leonard V, Day L. Educating nurses: a call for radical transformation. San Francisco: Jossey-Bass; 2010.
5. Jeffries PR. Simulation in nursing education: from conceptualization to evaluation. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2022.
6. Wartman SA, Combs CD. Reimagining medical education in the age of artificial intelligence. Academic Medicine. 2023;98(1):66-71. [https://doi.org/10.1097/ACM.0000000000004533] [PMID]
7. Bajwa J, Munir U, Nori A, Williams B. Artificial intelligence in healthcare: transforming the practice of medicine. Future Healthcare Journal. 2021;8(2):e188-e194. [https://doi.org/10.7861/fhj.2021-0095] [PMID]
8. Foronda CL, Fernandez-Burgos M, Nadeau C, Kelley CN, Henry MN. Virtual simulation in nursing education: a systematic review spanning 1996 to 2018. Simulation in Healthcare. 2020;15(1):46-54. [https://doi.org/10.1097/SIH.0000000000000411] [PMID]
9. Cook DA, Triola MM. Virtual patients: a critical literature review and proposed next steps. Medical Education. 2020;54(9):786-795. [https://doi.org/10.1111/medu.14172] [PMID]
10. Padilha JM, Machado PP, Ribeiro A, Ramos J, Costa P. Clinical virtual simulation in nursing education: randomized controlled trial. Journal of Medical Internet Research. 2021;23(3):e25466. [https://doi.org/10.2196/25466] [PMID]
11. Kardong-Edgren S, Farra SL, Alinier G, Young HM. Using virtual reality and augmented reality in nursing and medical education: a call for action. Clinical Simulation in Nursing. 2021;50:1-4. [https://doi.org/10.1016/j.ecns.2020.12.002]
12. Chen FQ, Leng YF, Ge JF, Wang DW, Li C, Chen B. Effectiveness of artificial intelligence in nursing education: a systematic review and meta-analysis. Nurse Education Today. 2024;135:106118. [https://doi.org/10.1016/j.nedt.2024.106118] [PMID]
13. Han ER, Yeo S, Kim MJ, Lee YH, Park KH, Roh H. The use of artificial intelligence in medical education: a systematic review and meta-analysis. PLOS ONE. 2023;18(5):e0285982. [https://doi.org/10.1371/journal.pone.0285982] [PMID]
14. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. [https://doi.org/10.1136/bmj.n71] [PMID]
15. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. [https://doi.org/10.1136/bmj.l4898] [PMID]
16. Kolb DA. Experiential learning: experience as the source of learning and development. 2nd ed. Upper Saddle River: FT Press; 2014.
17. Lapkin S, Levett-Jones T, Bellchambers H, Fernandez R. Effectiveness of patient simulation manikins in teaching clinical reasoning skills to undergraduate nursing students: a systematic review. Clinical Simulation in Nursing. 2021;46:1-14. [https://doi.org/10.1016/j.ecns.2020.08.010]
18. Hattie J, Timperley H. The power of feedback. Review of Educational Research. 2007;77(1):81-112. [https://doi.org/10.3102/003465430298487]
19. Sweller J, van Merriënboer JJG, Paas F. Cognitive architecture and instructional design: 20 years later. Educational Psychology Review. 2019;31(2):261-292. [https://doi.org/10.1007/s10648-019-09465-5]
20. Reason J. Managing the risks of organizational accidents. London: Routledge; 2016. [https://doi.org/10.4324/9781315543543]
21. O'Neill T, Lopes S. Error management training: a review and meta-analysis. Journal of Applied Psychology. 2022;107(12):2157-2184. [https://doi.org/10.1037/apl0001021] [PMID]
22. Shorey S, Ng ED. The use of virtual reality simulation among nursing students and registered nurses: a systematic review. Nurse Education Today. 2021;98:104662. [https://doi.org/10.1016/j.nedt.2020.104662] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |