
Preventive Care in Nursing and Midwifery Journal

Volume 15, Issue 2 (4-2025)
Prev Care Nurs Midwifery J 2025, 15(2): 13-22 |
Back to browse issues page

Ethics code: IR.ZUMS.REC. 1400.226
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Aligholipour M, Ramezani-Badr F, Hanifi N, Hormati Oghol Beig Z, Khezerlou Z. Examining the relationship between moral sensitivity and compassion satisfaction and fatigue among icu nurses: A correlational study. Prev Care Nurs Midwifery J 2025; 15 (2) :13-22
URL: http://nmcjournal.zums.ac.ir/article-1-989-en.html
URL: http://nmcjournal.zums.ac.ir/article-1-989-en.html
Mahtab Aligholipour  , Farhad Ramezani-Badr * , Nasrin Hanifi , Zahra Hormati Oghol Beig , Zahra Khezerlou
, Farhad Ramezani-Badr * , Nasrin Hanifi , Zahra Hormati Oghol Beig , Zahra Khezerlou
, Farhad Ramezani-Badr * , Nasrin Hanifi , Zahra Hormati Oghol Beig , Zahra Khezerlou
Associate Professor, Department of Critical Care and Emergency Nursing, School of Nursing and Midwifery, Zanjan University of Medical Sciences, Zanjan, Iran. , Ramezanibadr@gmail.com
Keywords: Moral Sensitivity, Compassion Satisfaction, Compassion Fatigue, Professional Quality of Life
Full-Text [PDF 746 kb]
(347 Downloads)
| Abstract (HTML) (1053 Views)
Statistical Methods
Data were analyzed using SPSS version 22. Descriptive statistics (mean, standard deviation, minimum, and maximum) were used to describe demographic characteristics. Inferential statistics were used to test hypotheses. The Kolmogorov–Smirnov test confirmed data normality (p > 0.05). The Pearson correlation coefficient was used to assess relationships between moral sensitivity and the dimensions of professional quality of life.
Results
The findings showed that the majority of the study participants were female (72.6%), married (93.2%), aged between 30 and 40 years (43.2%), and held a bachelor’s degree in nursing (73.3%). In addition, the highest frequency of participants belonged to permanent staff working in ICU units with less than five years of work experience (Table 1).
Table 1. Sociodemographic and Occupational Characteristics of Nurses (N = 146)
Note. ICU = Intensive Care Unit; CCU = Coronary Care Unit; NICU = Neonatal Intensive Care Unit.
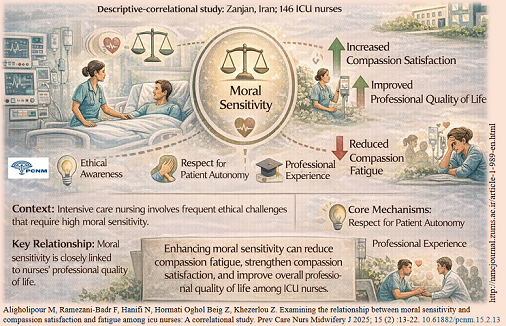
The mean scores of the moral sensitivity subscales, calculated based on a 4-point Likert scale, were as follows in descending order: Awareness of Communication (3.67), Ethical Decision-Making (3.43), Honesty (3.41), Moral Experience (3.23), Respect for Patient Autonomy (3.18), and Professional Knowledge (2.97) (Table 2). Moreover, 81.5% of participants demonstrated a high level of moral sensitivity (Table 3).
The results also indicated that the highest frequency of participants fell within the moderate level of compassion satisfaction (55.5%), while the highest level of compassion fatigue was observed in the high category (60.3%). The mean) standard deviation (for compassion satisfaction and compassion fatigue were 36.73 (SD= 6.12) and 65.02 (SD= 14.55), respectively (Table 4).
Inferential analyses revealed a positive and significant correlation between moral sensitivity and compassion satisfaction among nurses (R = 0.345, p < 0.05), whereas there was a negative and significant correlation between moral sensitivity and compassion fatigue (R = –0.321, p < 0.05). Furthermore, the subscales of respect for patient autonomy, professional knowledge, ethical decision-making, and honesty showed positive and significant correlations with compassion satisfaction. In contrast, the components of respect for patient autonomy and communication awareness demonstrated negative and significant correlations with compassion fatigue (p < 0.05) (Table 5)
Analysis of the subscales showed that “awareness of communication” had the highest mean score, while “professional knowledge” received the lowest. These results are consistent with previous studies, such as that by Farastkish et al. (2015) [25], whereas Sadrollahi et al. (2015) reported the highest score in “professional knowledge” and the lowest in “honesty and benevolence” [34], and Abbaszadeh et al. (2010) found the lowest score in “experience of ethical problems” and the highest in “professional knowledge” [35]. These discrepancies may arise from differences in cultural background, organizational structure, and educational approaches. They may also be related to environmental conditions, variations in ethics education, or hospital management policies. Specifically, in Zanjan’s educational hospitals, the lack of structured educational opportunities in professional ethics may explain the relatively lower score in the professional knowledge dimension.
Results related to compassion satisfaction indicated that although the mean score of this index was above average, less than half of the nurses reported a desirable level of satisfaction. This finding is similar to that of Mozafari et al. (2019) [36], suggesting that compassion satisfaction can play an important role in motivating nurses to continue providing care even under occupational stress. Conversely, the findings showed that more than 60% of nurses experienced a high level of compassion fatigue. This result aligns with national research by Mohammadi et al. (2015) and international studies by Ye (2024) and Maytum et al., indicating a high workload, staff shortage, and continuous emotional pressure in critical care units [37-39]. Global evidence also suggests that ICU nurses are more vulnerable to compassion fatigue than other professional groups due to the intensity of occupational stressors [40].
Analytical findings indicated a positive and significant relationship between moral sensitivity and compassion satisfaction, whereas an inverse relationship was observed between moral sensitivity and compassion fatigue. These results are consistent with the studies of Azadehjou et al. (2017) [15] and Hinderer [18]. It appears that moral sensitivity, by enhancing nurses’ ability to recognize ethical situations and reduce internal conflicts, contributes to increased satisfaction and reduced burnout. However, it should be noted that these findings indicate correlation only and cannot establish causation. Moreover, mediating factors such as psychological resilience, organizational support, and nurses’ personality traits may influence this relationship [41].
Based on the results obtained, it appears that enhancing moral sensitivity can play a vital role in improving nurses’ professional quality of life. Nevertheless, to gain a deeper understanding of how different dimensions of moral sensitivity interact with the components of compassion satisfaction and fatigue, further research is required. Future studies are recommended to examine the effects of educational interventions in professional ethics, organizational factors, and individual characteristics on this relationship. Additionally, longitudinal and interventional studies can help identify causal links and inform the design of effective programs to promote the psychological and professional well-being of ICU nurses.
Since the research instruments were self-reported, there is a possibility of response bias. To minimize this limitation, data were collected at appropriate times, and participants were provided with sufficient explanations about the importance, necessity, and objectives of the study. Moreover, the use of convenience sampling may increase the risk of selection bias; however, efforts were made to mitigate this by determining appropriate inclusion criteria and ensuring an adequate sample size among ICU nurses.
Conclusion
The results of the present study showed that the moral sensitivity of ICU nurses had a positive relationship with compassion satisfaction and an inverse, significant relationship with compassion fatigue. In other words, an increase in moral sensitivity enhances compassion satisfaction while reducing compassion fatigue. Moreover, various dimensions of moral sensitivity, including respect for patient autonomy, professional knowledge, ethical decision-making, and honesty, were associated with higher compassion satisfaction and lower emotional exhaustion, indicating that strengthening these competencies can act as a protective factor against occupational stress and ethical conflicts. From a clinical perspective, enhancing moral sensitivity through professional ethics education, organizational support, and reinforcement of nurses’ psychological resilience can improve the quality of care, nurse–patient communication, occupational resilience, and professional satisfaction, while simultaneously preventing the adverse consequences of compassion fatigue. Therefore, moral sensitivity should be recognized as a key competency in intensive care settings.
Ethical Considerations
This study was conducted in full compliance with ethical standards and was approved by the Ethics Committee of Zanjan University of Medical Sciences (Ethics Code: IR.ZUMS.REC.1400.226). Participation in the study was completely voluntary, and participants were allowed to withdraw at any stage of the research.
Written informed consent was obtained from all participants. The confidentiality of participants’ information was strictly maintained, and they were requested not to disclose their names on the questionnaires.
Funding
This research was supported by the Vice-Chancellery for Research and Technology of Zanjan University of Medical Sciences.
Conflict of Interest
Considering that the third author served as the editor-in-chief of the PCNM Journal, the peer review of this manuscript was conducted in the same manner as for other submissions, and the final decision regarding the article was made by the journal’s editorial board.
Acknowledgments
The authors would like to express their sincere appreciation to all the nurses who participated in this study for their valuable cooperation and contribution.
Authors' Contributions
Aligholipour M: Writing the manuscript and contributing to data analysis
Ramezani-Badr F: Contributing to data analysis, manuscript writing, and reviewing
Hanifi N: Data analysis, reviewing, and contributing to manuscript writing
Hormati Oghol Beig Z: Data collection, Contributing to data analysis,
Khezerlou Z: Writing the manuscript and contributing to data analysis
Artificial Intelligence Utilization for Article Writing
Artificial intelligence was utilized to enhance the fluency and coherence of the English text.
Data Availability Statement
The data are available from the corresponding author
Knowledge Translation Statement
Audience: Nurse managers, hospital administrators, ethics educators, and clinical supervisors in critical care settings.
Higher moral sensitivity in ICU nurses is significantly linked to greater compassion satisfaction and lower compassion fatigue. To leverage this, healthcare institutions should implement mandatory, continuous ethics training programs focusing on respect for patient autonomy, professional knowledge, and ethical decision-making. Additionally, creating supportive work environments and establishing peer support groups are recommended preventive strategies to reduce burnout and enhance nurses' professional quality of life.
Audience: Nurse managers, hospital administrators, ethics educators, and clinical supervisors in critical care settings.
Higher moral sensitivity in ICU nurses is significantly linked to greater compassion satisfaction and lower compassion fatigue. To leverage this, healthcare institutions should implement mandatory, continuous ethics training programs focusing on respect for patient autonomy, professional knowledge, and ethical decision-making. Additionally, creating supportive work environments and establishing peer support groups are recommended preventive strategies to reduce burnout and enhance nurses' professional quality of life.
Full-Text: (228 Views)
Introduction
Intensive Care Units (ICUs) are recognized as among the most sensitive and stressful environments in healthcare. Nurses working in these units constantly face unique challenges that affect their mental health and professional performance. The critical condition of patients, the need for rapid decision-making, and frequent exposure to death and dying make the ICU one of the most stressful clinical settings. Evidence indicates that nurses in these wards experience considerable psychological burden and occupational stress in emergencies such as cardiac arrest, managing critically ill patients, and providing end-of-life care [1-3]. Since nurses constitute the largest group of healthcare providers, their performance profoundly impacts the quality and outcomes of healthcare services. It can significantly contribute to the physical and psychological improvement and prognosis of patients in critical care [4,5].
In addition to possessing advanced technical and professional skills, ICU nurses need to demonstrate a high level of moral sensitivity [6]. Moral sensitivity is the ability to recognize moral situations and respond appropriately, playing a crucial role in ethical decision-making and the delivery of high-quality care. It encompasses components such as awareness of the moral dimensions of situations, responsibility, tolerance, and composure in the face of ethical challenges, and valuing ethical considerations in care provision. Moral sensitivity may play a central role in mitigating the negative effects of stressful ICU environments and assist nurses in better managing everyday ethical challenges [7].
Studies have shown that Intensive Care Nurses (ICNs) generally operate at moderate to high levels of moral sensitivity, and factors such as work experience, professional ethics education, and empathy skills can influence this sensitivity [7,8]. Research indicates that work experience, empathic ability, and organizational climate are among the main predictors of moral sensitivity in ICU nurses [6]. Moreover, the hospital's ethical climate strongly affects the professional quality of life of nurses, particularly those with specific personality traits [9]. Another study conducted among ICNs in Iran revealed that their moral sensitivity was moderate, and ethics education and work experience were the most significant predictors [10].
Nurses with higher levels of moral sensitivity tend to demonstrate better caring behaviors, greater respect for patients’ rights, and improved quality of care [11]. Beyond clinical outcomes, moral sensitivity has a substantial impact on nurses’ professional quality of life; specifically, nurses with higher moral sensitivity experience greater job satisfaction, lower burnout, and a stronger sense of meaning and value in their professional activities [12].
According to the Professional Quality of Life (ProQOL) model, professional quality of life includes three primary dimensions: compassion satisfaction, burnout, and secondary traumatic stress [13]. Compassion satisfaction refers to the positive feelings and fulfillment derived from effectively helping patients and alleviating their suffering. It includes aspects such as a sense of purpose and meaning in work, joy from making a positive difference in patients’ lives, and motivation and enthusiasm to continue working under challenging conditions [14]. Conversely, burnout refers to a state of physical, emotional, and psychological exhaustion resulting from prolonged exposure to occupational stressors, characterized by feelings of depleted energy, reduced personal accomplishment, cynicism, and emotional detachment from patients. Secondary traumatic stress, on the other hand, refers to psychological distress caused by repeated exposure to patients’ suffering, which may manifest as symptoms similar to post-traumatic stress disorder (PTSD) [13].
Research findings indicate that ICU nurses experience significantly higher levels of compassion fatigue, which includes both burnout and secondary traumatic stress, compared to nurses working in other hospital units [15,16]. Nurses in high-stress environments such as NICUs face substantial emotional and physical demands that lead to compassion fatigue, burnout, and secondary traumatic stress, severely impacting their professional quality of life [17]. These conditions may result in numerous negative outcomes, including reduced job performance, increased medical errors, decreased quality of patient care, higher absenteeism, and ultimately a greater intention to leave the profession [18]. Conversely, compassion satisfaction serves as a protective factor against such negative consequences and may be positively associated with nurses’ moral sensitivity [19].
Multiple studies have reported a significant relationship between moral sensitivity and the dimensions of nurses’ professional quality of life. In particular, compassion satisfaction, as the positive dimension of professional quality of life, is directly associated with higher levels of moral sensitivity [19, 20]. In contrast, burnout and secondary traumatic stress, which represent the negative dimensions, are generally linked to lower moral sensitivity [15].
Despite the existing research on the relationship between moral sensitivity and professional quality of life, considerable knowledge gaps remain in this area, particularly regarding ICU nurses in Iran, and few studies have explored these associations in depth. Furthermore, previous studies have not comprehensively examined how different dimensions of moral sensitivity relate to professional quality of life within organizational and environmental contexts such as the ICU. Investigating these relationships can provide valuable insights for improving professional performance and human resource management in these units, especially since ICU nurses face unique circumstances and ethical challenges requiring special attention.
Objectives
This study was designed to examine the relationship between moral sensitivity and the three dimensions of professional quality of life among ICU nurses working in educational hospitals in Zanjan, Iran. The findings of this research may enhance understanding of the interplay between these variables and inform the design of appropriate interventions aimed at promoting moral sensitivity and improving nurses’ professional quality of life. Additionally, the results can assist health policymakers in developing supportive programs for ICU nurses.
Materials and Methods
Study Design and Setting
This descriptive–correlational study was conducted in the intensive care units (ICU, CCU, and NICU) of educational hospitals affiliated with Zanjan University of Medical Sciences (Ayatollah Mousavi and Valiasr Hospitals) during 2021–2022.
Participants
The study population consisted of all nurses working in the intensive care units (CCU, ICU, and NICU) of these hospitals. The inclusion criteria consisted of having at least one year of work experience in an intensive care unit and a willingness to participate in the study voluntarily. The exclusion criteria included having psychological disorders and a lack of willingness to participate in the study.
Sampling Methods and Sample Size
A convenience sampling method was employed. The sample size was determined using the sample size formula for estimating the correlation between two variables, resulting in a total of 146 participants. The correlation coefficient of r = 0.729 from the study by Azadehjou et al. [15], which examined the relationship between moral sensitivity and professional quality of life among nurses, was used as the initial estimate. However, since this correlation was relatively high and could lead to an unrealistically small sample size, the final sample size was set between 120 and 150 participants to ensure adequate statistical power. Inclusion criteria were: Willingness to participate in the study, Possession of a Bachelor’s or Master’s degree in nursing, A minimum of one year of work experience in ICU, CCU, or NICU.
Data Collection Tools
Data were collected using three instruments: the Demographic questionnaire, Modified Moral Sensitivity Questionnaire (MMSQ) by Lützén et al. (1994), and Professional Quality of Life Scale (ProQOL) by Stamm and Figley (1990).
Demographic Questionnaire
This form collected information on gender, age, marital status, education level, employment status, work experience, work shift, and the specific intensive care unit of employment.
Modified Moral Sensitivity Questionnaire (MMSQ)
Moral sensitivity was measured using the modified version of Lützén’s Moral Sensitivity Questionnaire (MMSQ) [21], consisting of 25 items rated on a 5-point Likert scale (0 = neutral, 1 = strongly disagree, 2 = somewhat disagree, 3 = somewhat agree, 4 = strongly agree). The total score ranges from 0 to 100, with higher scores indicating greater moral sensitivity. 0–50: Low moral sensitivity, 51–75: Moderate moral sensitivity, 76–100: High moral sensitivity. The questionnaire includes six subscales: Respect for patient autonomy (score range: 0–12), Communication awareness (0–20), Professional knowledge (0–8), Experience of ethical problems and dilemmas (0–12), Application of ethical concepts in decision-making (0–20), Honesty and benevolence (0–28).
The validity and reliability of the original scale were confirmed by expert review and intraclass correlation analysis. In Iran, Mostafavian et al. (2019) confirmed its content validity and reported a Cronbach’s alpha of 0.79 [22]. In the present study, the Cronbach’s alpha coefficient was 0.88 for the total scale, and 0.79, 0.71, 0.78, 0.80, 0.73, and 0.76 for the six subscales, respectively, indicating acceptable internal consistency.
Professional Quality of Life Scale (ProQOL)
The ProQOL, developed by Stamm and Figley (1990), measures three dimensions: Compassion Satisfaction, Burnout, and Secondary Traumatic Stress. It contains 30 items rated on a 5-point Likert scale (1 = never to 5 = very often). Each subscale includes 10 items. Two subscales, burnout and secondary traumatic stress, constitute the components of compassion fatigue. The total possible score for compassion fatigue ranges from 20 to 100, while the range for compassion satisfaction is 10 to 50 [13]. Compassion satisfaction: 10–22 (low), 23–41 (moderate), 42–50 (high), Compassion fatigue: 20–47 (low), 48–75 (moderate), 76–100 (high).
Validity of the Persian version was confirmed by Gorji et al. (2015) [23] through exploratory and confirmatory factor analyses, and reliability by test–retest and internal consistency methods (Cronbach’s α = 0.73). In the current study, content validity was re-evaluated by ten nursing and ethics experts (CVR = 0.82) to ensure cultural and contextual suitability for Iranian ICU nurses. Reliability analysis yielded Cronbach’s α = 0.86 for the overall scale and 0.82, 0.79, and 0.75 for compassion satisfaction, burnout, and secondary traumatic stress, respectively, indicating strong internal consistency.
Data Collection Procedure
After obtaining ethical approval from the Ethics Committee of Zanjan University of Medical Sciences, eligible participants were recruited according to the inclusion criteria. Written informed consent was obtained before data collection. Participants were informed about the purpose of the study and assured of confidentiality and anonymity. They were asked to carefully complete the questionnaires (demographic form, MMSQ, and ProQOL). The completed questionnaires were collected and prepared for data analysis.
Variables
Intensive Care Units (ICUs) are recognized as among the most sensitive and stressful environments in healthcare. Nurses working in these units constantly face unique challenges that affect their mental health and professional performance. The critical condition of patients, the need for rapid decision-making, and frequent exposure to death and dying make the ICU one of the most stressful clinical settings. Evidence indicates that nurses in these wards experience considerable psychological burden and occupational stress in emergencies such as cardiac arrest, managing critically ill patients, and providing end-of-life care [1-3]. Since nurses constitute the largest group of healthcare providers, their performance profoundly impacts the quality and outcomes of healthcare services. It can significantly contribute to the physical and psychological improvement and prognosis of patients in critical care [4,5].
In addition to possessing advanced technical and professional skills, ICU nurses need to demonstrate a high level of moral sensitivity [6]. Moral sensitivity is the ability to recognize moral situations and respond appropriately, playing a crucial role in ethical decision-making and the delivery of high-quality care. It encompasses components such as awareness of the moral dimensions of situations, responsibility, tolerance, and composure in the face of ethical challenges, and valuing ethical considerations in care provision. Moral sensitivity may play a central role in mitigating the negative effects of stressful ICU environments and assist nurses in better managing everyday ethical challenges [7].
Studies have shown that Intensive Care Nurses (ICNs) generally operate at moderate to high levels of moral sensitivity, and factors such as work experience, professional ethics education, and empathy skills can influence this sensitivity [7,8]. Research indicates that work experience, empathic ability, and organizational climate are among the main predictors of moral sensitivity in ICU nurses [6]. Moreover, the hospital's ethical climate strongly affects the professional quality of life of nurses, particularly those with specific personality traits [9]. Another study conducted among ICNs in Iran revealed that their moral sensitivity was moderate, and ethics education and work experience were the most significant predictors [10].
Nurses with higher levels of moral sensitivity tend to demonstrate better caring behaviors, greater respect for patients’ rights, and improved quality of care [11]. Beyond clinical outcomes, moral sensitivity has a substantial impact on nurses’ professional quality of life; specifically, nurses with higher moral sensitivity experience greater job satisfaction, lower burnout, and a stronger sense of meaning and value in their professional activities [12].
According to the Professional Quality of Life (ProQOL) model, professional quality of life includes three primary dimensions: compassion satisfaction, burnout, and secondary traumatic stress [13]. Compassion satisfaction refers to the positive feelings and fulfillment derived from effectively helping patients and alleviating their suffering. It includes aspects such as a sense of purpose and meaning in work, joy from making a positive difference in patients’ lives, and motivation and enthusiasm to continue working under challenging conditions [14]. Conversely, burnout refers to a state of physical, emotional, and psychological exhaustion resulting from prolonged exposure to occupational stressors, characterized by feelings of depleted energy, reduced personal accomplishment, cynicism, and emotional detachment from patients. Secondary traumatic stress, on the other hand, refers to psychological distress caused by repeated exposure to patients’ suffering, which may manifest as symptoms similar to post-traumatic stress disorder (PTSD) [13].
Research findings indicate that ICU nurses experience significantly higher levels of compassion fatigue, which includes both burnout and secondary traumatic stress, compared to nurses working in other hospital units [15,16]. Nurses in high-stress environments such as NICUs face substantial emotional and physical demands that lead to compassion fatigue, burnout, and secondary traumatic stress, severely impacting their professional quality of life [17]. These conditions may result in numerous negative outcomes, including reduced job performance, increased medical errors, decreased quality of patient care, higher absenteeism, and ultimately a greater intention to leave the profession [18]. Conversely, compassion satisfaction serves as a protective factor against such negative consequences and may be positively associated with nurses’ moral sensitivity [19].
Multiple studies have reported a significant relationship between moral sensitivity and the dimensions of nurses’ professional quality of life. In particular, compassion satisfaction, as the positive dimension of professional quality of life, is directly associated with higher levels of moral sensitivity [19, 20]. In contrast, burnout and secondary traumatic stress, which represent the negative dimensions, are generally linked to lower moral sensitivity [15].
Despite the existing research on the relationship between moral sensitivity and professional quality of life, considerable knowledge gaps remain in this area, particularly regarding ICU nurses in Iran, and few studies have explored these associations in depth. Furthermore, previous studies have not comprehensively examined how different dimensions of moral sensitivity relate to professional quality of life within organizational and environmental contexts such as the ICU. Investigating these relationships can provide valuable insights for improving professional performance and human resource management in these units, especially since ICU nurses face unique circumstances and ethical challenges requiring special attention.
Objectives
This study was designed to examine the relationship between moral sensitivity and the three dimensions of professional quality of life among ICU nurses working in educational hospitals in Zanjan, Iran. The findings of this research may enhance understanding of the interplay between these variables and inform the design of appropriate interventions aimed at promoting moral sensitivity and improving nurses’ professional quality of life. Additionally, the results can assist health policymakers in developing supportive programs for ICU nurses.
Materials and Methods
Study Design and Setting
This descriptive–correlational study was conducted in the intensive care units (ICU, CCU, and NICU) of educational hospitals affiliated with Zanjan University of Medical Sciences (Ayatollah Mousavi and Valiasr Hospitals) during 2021–2022.
Participants
The study population consisted of all nurses working in the intensive care units (CCU, ICU, and NICU) of these hospitals. The inclusion criteria consisted of having at least one year of work experience in an intensive care unit and a willingness to participate in the study voluntarily. The exclusion criteria included having psychological disorders and a lack of willingness to participate in the study.
Sampling Methods and Sample Size
A convenience sampling method was employed. The sample size was determined using the sample size formula for estimating the correlation between two variables, resulting in a total of 146 participants. The correlation coefficient of r = 0.729 from the study by Azadehjou et al. [15], which examined the relationship between moral sensitivity and professional quality of life among nurses, was used as the initial estimate. However, since this correlation was relatively high and could lead to an unrealistically small sample size, the final sample size was set between 120 and 150 participants to ensure adequate statistical power. Inclusion criteria were: Willingness to participate in the study, Possession of a Bachelor’s or Master’s degree in nursing, A minimum of one year of work experience in ICU, CCU, or NICU.
Data Collection Tools
Data were collected using three instruments: the Demographic questionnaire, Modified Moral Sensitivity Questionnaire (MMSQ) by Lützén et al. (1994), and Professional Quality of Life Scale (ProQOL) by Stamm and Figley (1990).
Demographic Questionnaire
This form collected information on gender, age, marital status, education level, employment status, work experience, work shift, and the specific intensive care unit of employment.
Modified Moral Sensitivity Questionnaire (MMSQ)
Moral sensitivity was measured using the modified version of Lützén’s Moral Sensitivity Questionnaire (MMSQ) [21], consisting of 25 items rated on a 5-point Likert scale (0 = neutral, 1 = strongly disagree, 2 = somewhat disagree, 3 = somewhat agree, 4 = strongly agree). The total score ranges from 0 to 100, with higher scores indicating greater moral sensitivity. 0–50: Low moral sensitivity, 51–75: Moderate moral sensitivity, 76–100: High moral sensitivity. The questionnaire includes six subscales: Respect for patient autonomy (score range: 0–12), Communication awareness (0–20), Professional knowledge (0–8), Experience of ethical problems and dilemmas (0–12), Application of ethical concepts in decision-making (0–20), Honesty and benevolence (0–28).
The validity and reliability of the original scale were confirmed by expert review and intraclass correlation analysis. In Iran, Mostafavian et al. (2019) confirmed its content validity and reported a Cronbach’s alpha of 0.79 [22]. In the present study, the Cronbach’s alpha coefficient was 0.88 for the total scale, and 0.79, 0.71, 0.78, 0.80, 0.73, and 0.76 for the six subscales, respectively, indicating acceptable internal consistency.
Professional Quality of Life Scale (ProQOL)
The ProQOL, developed by Stamm and Figley (1990), measures three dimensions: Compassion Satisfaction, Burnout, and Secondary Traumatic Stress. It contains 30 items rated on a 5-point Likert scale (1 = never to 5 = very often). Each subscale includes 10 items. Two subscales, burnout and secondary traumatic stress, constitute the components of compassion fatigue. The total possible score for compassion fatigue ranges from 20 to 100, while the range for compassion satisfaction is 10 to 50 [13]. Compassion satisfaction: 10–22 (low), 23–41 (moderate), 42–50 (high), Compassion fatigue: 20–47 (low), 48–75 (moderate), 76–100 (high).
Validity of the Persian version was confirmed by Gorji et al. (2015) [23] through exploratory and confirmatory factor analyses, and reliability by test–retest and internal consistency methods (Cronbach’s α = 0.73). In the current study, content validity was re-evaluated by ten nursing and ethics experts (CVR = 0.82) to ensure cultural and contextual suitability for Iranian ICU nurses. Reliability analysis yielded Cronbach’s α = 0.86 for the overall scale and 0.82, 0.79, and 0.75 for compassion satisfaction, burnout, and secondary traumatic stress, respectively, indicating strong internal consistency.
Data Collection Procedure
After obtaining ethical approval from the Ethics Committee of Zanjan University of Medical Sciences, eligible participants were recruited according to the inclusion criteria. Written informed consent was obtained before data collection. Participants were informed about the purpose of the study and assured of confidentiality and anonymity. They were asked to carefully complete the questionnaires (demographic form, MMSQ, and ProQOL). The completed questionnaires were collected and prepared for data analysis.
Variables
- Independent variable: Moral sensitivity (total and subscales)
- Dependent variables: Compassion satisfaction and compassion fatigue (burnout and secondary traumatic stress)
Statistical Methods
Data were analyzed using SPSS version 22. Descriptive statistics (mean, standard deviation, minimum, and maximum) were used to describe demographic characteristics. Inferential statistics were used to test hypotheses. The Kolmogorov–Smirnov test confirmed data normality (p > 0.05). The Pearson correlation coefficient was used to assess relationships between moral sensitivity and the dimensions of professional quality of life.
Results
The findings showed that the majority of the study participants were female (72.6%), married (93.2%), aged between 30 and 40 years (43.2%), and held a bachelor’s degree in nursing (73.3%). In addition, the highest frequency of participants belonged to permanent staff working in ICU units with less than five years of work experience (Table 1).
Table 1. Sociodemographic and Occupational Characteristics of Nurses (N = 146)
| Characteristic | Category | n | % |
| Gender | Male | 40 | 27.4 |
| Female | 106 | 72.6 | |
| Age (years) | <30 | 57 | 39.0 |
| 30–40 | 63 | 43.2 | |
| >40 | 26 | 17.8 | |
| Marital status | Single | 10 | 6.8 |
| Married | 136 | 93.2 | |
| Education | Associate | 11 | 7.5 |
| Bachelor | 107 | 73.3 | |
| Master | 28 | 19.2 | |
| Employment type | Official | 58 | 39.7 |
| Contractual | 57 | 39.0 | |
| Temporary | 28 | 19.2 | |
| Internship | 3 | 2.1 | |
| Work experience | <5 years | 74 | 50.7 |
| 5–10 years | 61 | 41.8 | |
| >10 years | 11 | 7.5 | |
| Shift | Morning | 35 | 24.0 |
| Evening | 29 | 19.9 | |
| Night | 7 | 4.8 | |
| Rotating | 75 | 51.3 | |
| Clinical unit | ICU | 70 | 47.9 |
| CCU | 58 | 39.7 | |
| NICU | 18 | 12.4 |
The mean scores of the moral sensitivity subscales, calculated based on a 4-point Likert scale, were as follows in descending order: Awareness of Communication (3.67), Ethical Decision-Making (3.43), Honesty (3.41), Moral Experience (3.23), Respect for Patient Autonomy (3.18), and Professional Knowledge (2.97) (Table 2). Moreover, 81.5% of participants demonstrated a high level of moral sensitivity (Table 3).
The results also indicated that the highest frequency of participants fell within the moderate level of compassion satisfaction (55.5%), while the highest level of compassion fatigue was observed in the high category (60.3%). The mean) standard deviation (for compassion satisfaction and compassion fatigue were 36.73 (SD= 6.12) and 65.02 (SD= 14.55), respectively (Table 4).
Inferential analyses revealed a positive and significant correlation between moral sensitivity and compassion satisfaction among nurses (R = 0.345, p < 0.05), whereas there was a negative and significant correlation between moral sensitivity and compassion fatigue (R = –0.321, p < 0.05). Furthermore, the subscales of respect for patient autonomy, professional knowledge, ethical decision-making, and honesty showed positive and significant correlations with compassion satisfaction. In contrast, the components of respect for patient autonomy and communication awareness demonstrated negative and significant correlations with compassion fatigue (p < 0.05) (Table 5)
Table 2. Descriptive Statistics of Overall Moral Sensitivity and Its Subscales among Study Participants (N = 146)
| Variable | Mean | SD | Minimum | Maximum | Relative Score | |
| Mean | SD | |||||
| Moral Sensitivity | 87.18 | 5.51 | 71 | 98 | — | — |
| Respect for Patient Autonomy | 9.54 | 2.53 | 3 | 12 | 3.18 | 0.84 |
| Awareness of Communication | 18.40 | 1.47 | 14 | 20 | 3.67 | 0.30 |
| Professional Knowledge | 5.96 | 1.74 | 2 | 8 | 2.97 | 0.87 |
| Moral Experience | 9.71 | 1.51 | 6 | 12 | 3.23 | 0.51 |
| Ethical Decision-Making | 17.18 | 1.84 | 10 | 20 | 3.43 | 0.37 |
| Honesty | 23.90 | 2.66 | 16 | 28 | 3.41 | 0.38 |
Table 3. Distribution of Moral Sensitivity Levels Among ICU Nurses (N = 146)
Discussion
The findings of the present study showed that the mean score of moral sensitivity among nurses working in the intensive care units (ICUs) of educational hospitals in Zanjan was above average, and 81.5% of nurses reported a high level of moral sensitivity. This finding is consistent with many national and international studies, including those by Beghaei [24], Farastkish [25], and Momen-Nasab [26]. A recent meta-analysis also reported the moral sensitivity of Iranian nurses within the moderate to moderately high range, accompanied by regional and interprovincial variations [27]. Another study conducted among ICU nurses in Iran revealed that moral sensitivity had an inverse relationship with compassion fatigue and could play a protective role [10].
Previous studies have shown that moral sensitivity among ICU nurses is directly and significantly associated with their ability to make ethical decisions in critical situations, such that strengthening this sensitivity leads to a reduction in ethical conflicts [28]. The consistency of the findings may be attributed to the similar nature of the work environment, professional conditions, and shared awareness of ethical obligations among nurses. Moral sensitivity, as a complex behavioral construct encompassing perceptions, emotions, intentions, and actions, helps nurses identify patients’ problems on time and make optimal ethical decisions [29]. Previous evidence suggests that moral sensitivity improves ethical performance and enhances the quality of nurse–patient communication while reducing moral distress [26, 30]. Studies have also indicated that moral sensitivity among ICU nurses in Iran and other countries is generally at a desirable level [31, 32].
| Moral Sensitivity Level | n | % |
| Low (0–50) | 13 | 8.9 |
| Moderate (51–75) | 14 | 9.6 |
| High (76–100) | 119 | 81.5 |
| Total | 146 | 100 |
The findings of the present study showed that the mean score of moral sensitivity among nurses working in the intensive care units (ICUs) of educational hospitals in Zanjan was above average, and 81.5% of nurses reported a high level of moral sensitivity. This finding is consistent with many national and international studies, including those by Beghaei [24], Farastkish [25], and Momen-Nasab [26]. A recent meta-analysis also reported the moral sensitivity of Iranian nurses within the moderate to moderately high range, accompanied by regional and interprovincial variations [27]. Another study conducted among ICU nurses in Iran revealed that moral sensitivity had an inverse relationship with compassion fatigue and could play a protective role [10].
Previous studies have shown that moral sensitivity among ICU nurses is directly and significantly associated with their ability to make ethical decisions in critical situations, such that strengthening this sensitivity leads to a reduction in ethical conflicts [28]. The consistency of the findings may be attributed to the similar nature of the work environment, professional conditions, and shared awareness of ethical obligations among nurses. Moral sensitivity, as a complex behavioral construct encompassing perceptions, emotions, intentions, and actions, helps nurses identify patients’ problems on time and make optimal ethical decisions [29]. Previous evidence suggests that moral sensitivity improves ethical performance and enhances the quality of nurse–patient communication while reducing moral distress [26, 30]. Studies have also indicated that moral sensitivity among ICU nurses in Iran and other countries is generally at a desirable level [31, 32].
Table 4. Distribution of Compassion Satisfaction and Compassion Fatigue Levels among Study Participants (N = 146)
Note. The Mean and SD values represent the overall scores for each variable scale, not individual levels.
Table 5. Correlations between Moral Sensitivity and Compassion Satisfaction and Fatigue among ICU Nurses (N = 146)
The differing results of the study by Borhani et al. (2017), which reported a moderate level of moral sensitivity [33], may be due to differences in workplace settings and organizational conditions. Recent studies have shown that continuous professional ethics education can significantly enhance nurses’ moral sensitivity and strengthen their ability to make rapid ethical decisions in critical conditions [6].| Variable | Level | n | % | Mean | SD |
| Compassion Satisfaction | Low (10–22) | 6 | 4.1 | 73.36 | 12.6 |
| Moderate (23–41) | 81 | 55.5 | |||
| High (42–50) | 59 | 40.4 | |||
| Total | 146 | 100 | |||
| Compassion Fatigue | Low (20–47) | 31 | 21.2 | 65.02 | 14.55 |
| Moderate (48–75) | 27 | 18.5 | |||
| High (76–100) | 88 | 60.3 | |||
| Total | 146 | 100 |
Table 5. Correlations between Moral Sensitivity and Compassion Satisfaction and Fatigue among ICU Nurses (N = 146)
| Moral Sensitivity Subscale | Compassion Satisfaction | Compassion Fatigue | ||
| r | p | r | p | |
| Total Moral Sensitivity | 0.34 | < 0.001 | -0.21 | < 0.001 |
| Respect for Patient Autonomy | 0.35 | < 0.001 | -0.24 | 0.011 |
| Awareness of Communication | 0.06 | 0.435 | -0.21 | 0.011 |
| Professional Knowledge | 0.28 | <0.001 | -0.11 | 0.182 |
| Moral Experience | 0.05 | 0.479 | -0.09 | 0.239 |
| Ethical Decision-Making | 0.24 | < 0.001 | -0.10 | 0.191 |
| Honesty | 0.30 | <0.001 | 0.00 | 0.994 |
Analysis of the subscales showed that “awareness of communication” had the highest mean score, while “professional knowledge” received the lowest. These results are consistent with previous studies, such as that by Farastkish et al. (2015) [25], whereas Sadrollahi et al. (2015) reported the highest score in “professional knowledge” and the lowest in “honesty and benevolence” [34], and Abbaszadeh et al. (2010) found the lowest score in “experience of ethical problems” and the highest in “professional knowledge” [35]. These discrepancies may arise from differences in cultural background, organizational structure, and educational approaches. They may also be related to environmental conditions, variations in ethics education, or hospital management policies. Specifically, in Zanjan’s educational hospitals, the lack of structured educational opportunities in professional ethics may explain the relatively lower score in the professional knowledge dimension.
Results related to compassion satisfaction indicated that although the mean score of this index was above average, less than half of the nurses reported a desirable level of satisfaction. This finding is similar to that of Mozafari et al. (2019) [36], suggesting that compassion satisfaction can play an important role in motivating nurses to continue providing care even under occupational stress. Conversely, the findings showed that more than 60% of nurses experienced a high level of compassion fatigue. This result aligns with national research by Mohammadi et al. (2015) and international studies by Ye (2024) and Maytum et al., indicating a high workload, staff shortage, and continuous emotional pressure in critical care units [37-39]. Global evidence also suggests that ICU nurses are more vulnerable to compassion fatigue than other professional groups due to the intensity of occupational stressors [40].
Analytical findings indicated a positive and significant relationship between moral sensitivity and compassion satisfaction, whereas an inverse relationship was observed between moral sensitivity and compassion fatigue. These results are consistent with the studies of Azadehjou et al. (2017) [15] and Hinderer [18]. It appears that moral sensitivity, by enhancing nurses’ ability to recognize ethical situations and reduce internal conflicts, contributes to increased satisfaction and reduced burnout. However, it should be noted that these findings indicate correlation only and cannot establish causation. Moreover, mediating factors such as psychological resilience, organizational support, and nurses’ personality traits may influence this relationship [41].
Based on the results obtained, it appears that enhancing moral sensitivity can play a vital role in improving nurses’ professional quality of life. Nevertheless, to gain a deeper understanding of how different dimensions of moral sensitivity interact with the components of compassion satisfaction and fatigue, further research is required. Future studies are recommended to examine the effects of educational interventions in professional ethics, organizational factors, and individual characteristics on this relationship. Additionally, longitudinal and interventional studies can help identify causal links and inform the design of effective programs to promote the psychological and professional well-being of ICU nurses.
Since the research instruments were self-reported, there is a possibility of response bias. To minimize this limitation, data were collected at appropriate times, and participants were provided with sufficient explanations about the importance, necessity, and objectives of the study. Moreover, the use of convenience sampling may increase the risk of selection bias; however, efforts were made to mitigate this by determining appropriate inclusion criteria and ensuring an adequate sample size among ICU nurses.
Conclusion
The results of the present study showed that the moral sensitivity of ICU nurses had a positive relationship with compassion satisfaction and an inverse, significant relationship with compassion fatigue. In other words, an increase in moral sensitivity enhances compassion satisfaction while reducing compassion fatigue. Moreover, various dimensions of moral sensitivity, including respect for patient autonomy, professional knowledge, ethical decision-making, and honesty, were associated with higher compassion satisfaction and lower emotional exhaustion, indicating that strengthening these competencies can act as a protective factor against occupational stress and ethical conflicts. From a clinical perspective, enhancing moral sensitivity through professional ethics education, organizational support, and reinforcement of nurses’ psychological resilience can improve the quality of care, nurse–patient communication, occupational resilience, and professional satisfaction, while simultaneously preventing the adverse consequences of compassion fatigue. Therefore, moral sensitivity should be recognized as a key competency in intensive care settings.
Ethical Considerations
This study was conducted in full compliance with ethical standards and was approved by the Ethics Committee of Zanjan University of Medical Sciences (Ethics Code: IR.ZUMS.REC.1400.226). Participation in the study was completely voluntary, and participants were allowed to withdraw at any stage of the research.
Written informed consent was obtained from all participants. The confidentiality of participants’ information was strictly maintained, and they were requested not to disclose their names on the questionnaires.
Funding
This research was supported by the Vice-Chancellery for Research and Technology of Zanjan University of Medical Sciences.
Conflict of Interest
Considering that the third author served as the editor-in-chief of the PCNM Journal, the peer review of this manuscript was conducted in the same manner as for other submissions, and the final decision regarding the article was made by the journal’s editorial board.
Acknowledgments
The authors would like to express their sincere appreciation to all the nurses who participated in this study for their valuable cooperation and contribution.
Authors' Contributions
Aligholipour M: Writing the manuscript and contributing to data analysis
Ramezani-Badr F: Contributing to data analysis, manuscript writing, and reviewing
Hanifi N: Data analysis, reviewing, and contributing to manuscript writing
Hormati Oghol Beig Z: Data collection, Contributing to data analysis,
Khezerlou Z: Writing the manuscript and contributing to data analysis
Artificial Intelligence Utilization for Article Writing
Artificial intelligence was utilized to enhance the fluency and coherence of the English text.
Data Availability Statement
The data are available from the corresponding author
Type of Study: Orginal research |
Subject:
Nursing
References
1. Arries-Kleyenstuber E, Dierckx de Casterle B, Kynoch K, Ramis MA, Suhonen R, Ventura C, et al. Ethical Challenges Nurses Faced During the COVID-19 Pandemic: Scoping Review. Nursing Ethics. 2025;9697330251339417. [https://doi.org/10.1177/09697330251339417]
2. Atashzadeh-Shoorideh F, Tayyar-Iravanlou F, Chashmi ZA, Abdi F, Cisic RS. Factors Affecting Moral Distress in Nurses Working in Intensive Care Units: A Systematic Review. Clinical Ethics. 2020;16(1):25-36. [https://doi.org/10.1177/1477750920927174]
3. Marshall JC, Bosco L, Adhikari NK, Connolly B, Diaz JV, Dorman T, et al. What Is an Intensive Care Unit? A Report of the Task Force of the World Federation of Societies of Intensive and Critical Care Medicine. Journal of Critical Care. 2017;37:270-6. [https://doi.org/10.1016/j.jcrc.2016.07.015]
4. Karaca A, Durna Z. Patient Satisfaction With the Quality of Nursing Care. Nursing Open. 2019;6(2):535-45. [https://doi.org/10.1002/nop2.237]
5. Shalaby SA, Janbi NF, Mohammed KK, Al-harthi KM. Assessing the Caring Behaviors of Critical Care Nurses. Journal of Nursing Education and Practice. 2018;8(10):77-85. [https://doi.org/10.5430/jnep.v8n10p77]
6. Wang K, Mi Y, Wu Y, Sun H. Career Calling, Ethical Sensitivity, and Decision-Making Ability in Intensive Care Nurses: A Mediating Effect Model. Frontiers in Psychology. 2025;16:1512533. [https://doi.org/10.3389/fpsyg.2025.1512533]
7. Sharifnia AM, Green H, Fernandez R, Alananzeh I. Empathy and Ethical Sensitivity Among Intensive and Critical Care Nurses: A Path Analysis. Nursing Ethics. 2024;31(2-3):227-42. [https://doi.org/10.1177/09697330231167543]
8. İlter SM, Ovayolu Ö, Serçe S, Ovayolu N. An Investigation of the Relationship Between Compassion Fatigue and Moral Sensitivity of Intensive Care Nurses. Omega-Journal of Death and Dying. 2024;90(2):521-35. [https://doi.org/10.1177/00302228221107976]
9. Matsuishi Y, Mathis BJ, Hoshino H, Enomoto Y, Shimojo N, Kawano S, et al. PERSonality, Ehical, and PROfessional Quality of Life in Pediatric/Adult Intensive Nurses Study: PERSEPRO PAIN Study. PLoS One. 2022;17(3):e0259721. [https://doi.org/10.1371/journal.pone.0259721]
10. Babaei SM, Araghian Mojarrad F, Kamali M, Arab Larimi M, Jafari H. Moral Sensitivity and Related Factors in Iranian Critical Care Nurses: A Narrative Review. Journal of Nursing Reports in Clinical Practice. 2023;1(2):78-83. [https://doi.org/10.32598/JNRCP.23.42]
11. Nazari AM. Relationship Between Ethical Sensitivity and the Nurses’ Quality of Care: A Systematic Review. Iranian Biomedical Journal. 2024;28:439. [https://doi.org/10.61186/ibj.25th-11th-IACRTIMSS]
12. Rigi ZE, Fard SB, Saadatifar B, Miri M, Akbari O. The Relationship Between Moral Sensitivity, Moral Distress, Perceived Organizational Support, and Self‐Esteem in Iranian Nurses: A Cross‐Sectional Analytical Study. International Nursing Review. 2025;72(3):e70058. [https://doi.org/10.1111/inr.70058]
13. Stamm B. The Concise Manual for the Professional Quality of Life Scale. 2010.
14. Panagou E, Missouridou ED, Zartaloudi A, Koutelekos J, Dousis E, Dafogianni C, et al. Compassion Fatigue and Compassion Satisfaction in Pediatric Intensive Care Professionals. Materia Socio-Medica. 2023;35(1):28. [https://doi.org/10.5455/msm.2023.35.28-32]
15. Azadehjo N, Nasrabadi T, Nasrollah S. The Relationship of Compassion Fatigues and Moral Sensitivity in Critical Care Nurses. Iranian Journal of Cardiovascular Nursing. 2018;6(4):50-9. [http://journal.icns.org.ir/article-1-506-en.html]
16. Mazaheri Z, Sajjadian I. Structural Model of the Relationship of Empathic Concerns With Compassion Satisfaction and Compassion Fatigue in Intensive Care Units Nurses. 2019. [https://www.sid.ir/paper/363198/en]
17. Durgannavar MS, Sajjan MS, Natekar DS. A Correlational Study to Assess the Percieved Stress and Professional Quality of Life Among NICU Staff Nurses at Selected Hospitals of Bagalkot, With View to Develop an Interventional Package. Scholars Journal of Applied Medical Sciences. 2025;13(1):235-41. [https://doi.org/10.36347/sjams.2025.v13i01.037]
18. Hinderer KA, VonRueden KT, Friedmann E, McQuillan KA, Gilmore R, Kramer B, et al. Burnout, Compassion Fatigue, Compassion Satisfaction, and Secondary Traumatic Stress in Trauma Nurses. Journal of Trauma Nursing. 2014;21(4):160-9. [https://doi.org/10.1097/JTN.0000000000000055]
19. Karakoc Kumsar A, Polat S, Taskin Yilmaz F. The Effect on Ethical Sensitivity of Compassion Level in Nurses. Electronic Journal of General Medicine. 2021;18(5):em302. [https://doi.org/10.29333/ejgm/11011]
20. Bilgiç Ş. Does the Compassion Level of Nursing Students Affect Their Ethical Sensitivity? Nurse Education Today. 2022;109:105228. [https://doi.org/10.1016/j.nedt.2021.105228]
21. Lützén K, Nordin C, Brolin G. Conceptualization and Instrumentation of Nurses' Moral Sensitivity in Psychiatric Practice. International Journal of Methods in Psychiatric Research. 1994.
22. Mostafavian Z, Gholampour J, Faraj Pour A, Akbari Farmad S, Rahchamani MA. Comparison of Moral Sensitivity Among Last Year Nursing Students and Nurses Working at Teaching Hospitals of Islamic Azad University of Mashhad. Education and Ethics In Nursing. 2019;8(3-4):30-6. [https://doi.org/10.52547/ethicnurs.8.3.4.30]
23. Ghorji M, Keshavarz Z, Ebadi A, Nasiri M. Persian Translation and Psychometric Properties of Professional Quality of Life Scale (ProQOL) for Health Care Providers. Journal of Mazandaran University of Medical Sciences. 2018;28(163):93-106. [https://jmums.mazums.ac.ir/article-1-10095-en.html]
24. Baghaei R, Moradi Y, Aminolshareh S, Zareh H. The Ethical Sensitivity of Nurses in Decision Making in Ayatollah Taleghani Hospital, 1391. Nursing And Midwifery Journal. 2014;11(11). [https://unmf.umsu.ac.ir/article-1-1700-en.html]
25. Frastkish R. Investigating the Sensitivity of ICU Nurses in Shahid Rajaie Cardiovascular Center. Cardiovascular Nursing Journal. 2015;4(3):36-45.
26. Momennasab M, Homayoon Z, Torabizadeh C. Critical Care Nurses’ Adherence to Ethical Codes and Its Association With Spiritual Well‐Being and Moral Sensitivity. Critical Care Research and Practice. 2023;2023(1):8248948. [https://doi.org/10.1155/2023/8248948]
27. Ghanei Gheshlagh R, Dehvan F, Sedighi L. Moral Sensitivity in Iranian Nurses: Insights From a Nationwide Meta-Analysis. BMC Nursing. 2025;24(1):294. [https://doi.org/10.1186/s12912-025-02940-1]
28. He Q, Huang C, Feng Z, Shen H. The Relationships Between Ethical Sensitivity, Ethical Decision‐Making Ability, and Ethical Conflict Among ICU Nurses: A Structural Equation Model. Journal of Nursing Management. 2025;2025(1):7756343. [https://doi.org/10.1155/jonm/7756343]
29. Imani J, Rezae HH, Mirzai M. Evaluation the Effect of Work Conscientiousness and Moral Sensitivity With Ethical Stress in Nurses Working in Intensive Care Units in Educational and Therapeutic Centers Affiliated to Zahedan University of Medical Sciences. Quarterly Journal of Iranian Society Anaesthesiology and Intensive Care Quarterly. 2018;2(4):20-7.
30. Lützen K, Dahlqvist V, Eriksson S, Norberg A. Developing the Concept of Moral Sensitivity in Health Care Practice. Nursing Ethics. 2006;13(2):187-96. [https://doi.org/10.1191/0969733006ne837oa]
31. Khorani H, Momeni M, Ahmadi A, Motalebi SA. Predictive Value of Moral Sensitivity for Quality of Care Among Iranian Nurses. Jundishapur Journal of Chronic Disease Care. 2024;13(1). [https://doi.org/10.5812/jjcdc-138899]
32. Hojjati H, Koupaei SE, Madvar TR, Pour NH, Delavari A, Niya HM, et al. The Relationship Between Futile Care and Moral Sensitivity in Nurses Working in the Neonatal Intensive Care Unit of Medical Training Centers in Gorgan 2024. Archives of Anesthesiology and Critical Care. 2025. [https://doi.org/10.18502/aacc.v11i4.9373]
33. Borhani F, Abbaszadeh A, Mohamadi E, Ghasemi E, Hoseinabad-Farahani MJ. Moral Sensitivity and Moral Distress in Iranian Critical Care Nurses. Nursing Ethics. 2017;24(4):474-82. [https://doi.org/10.1177/0969733015604700]
34. Sadrollahi A, KZ. A Survey of Professional Moral Sensitivity and Associated Factors Among the Nurses in West Golestan Province of Iran. Iranian Journal of Medical Ethics and History of Medicine. 2015;8(3):50-61.
35. Abbaszadeh A, Borhani F, Moazen N. The Comparison of the Level of Moral Sensitivity in Nursing Students and Nursing Staffs in Kerman in 1389. Medical Ethics. 2010;4(12):39-54. [https://www.sid.ir/paper/195578/en]
36. Mazaheri Z, Sajjadian I. Structural Model of the Relationship of Empathic Concerns With Compassion Satisfaction and Compassion Fatigue in Intensive Care Units Nurses. Nursing And Midwifery Journal. 2019;17(1):62-70. [https://www.sid.ir/paper/363198/en]
37. Mohammady S. Self-Compassion in Critical Care Nurses. Faslname-i mudiriyyat-e parastari. 2016;5(2):44-50. [https://doi.org/10.29252/ijnv.5.2.44]
38. Ye L, Tang X, Li Y, Zhu Y, Shen J, Zhu Y, et al. The Prevalence and Related Factors of Compassion Fatigue Among Nursing Interns: A Cross-Sectional Study. BMC Nursing. 2024;23(1):762. [https://doi.org/10.1186/s12912-024-02384-z]
39. Maytum JC, Heiman MB, Garwick AW. Compassion Fatigue and Burnout in Nurses Who Work With Children With Chronic Conditions and Their Families. Journal of Pediatric Health Care. 2004;18(4):171-9. [https://doi.org/10.1016/j.pedhc.2003.12.005]
40. Xie W, Chen L, Feng F, Okoli CT, Tang P, Zeng L, et al. The Prevalence of Compassion Satisfaction and Compassion Fatigue Among Nurses: A Systematic Review and Meta-Analysis. International Journal of Nursing Studies. 2021;120:103973. [https://doi.org/10.1016/j.ijnurstu.2021.103973]
41. Liu D, Xie S, Jing J, Niyomsilp E, Xie L, Nie X, et al. The Effect of Perceived Organizational Support and Ego-Resilience on the Relationship Between Occupational Stressors and Compassion Fatigue in COVID-19 Frontline Nurses: A Cross-Sectional Study in Sichuan, China. BMC Nursing. 2024;23(1):817. [https://doi.org/10.1186/s12912-024-02473-z]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |