
Preventive Care in Nursing and Midwifery Journal

Volume 16, Issue 2 (4-2026)
Prev Care Nurs Midwifery J 2026, 16(2): 13-25 |
Back to browse issues page

Ethics code: IR.IAU.SRB.REC.1404.137
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
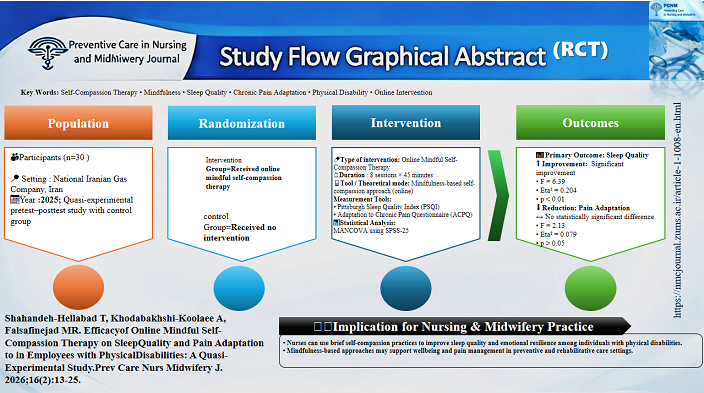
Shahaned-hellaba T, Khodabakhshi-Koolaee A, Falsafinejad M R. Efficacy of Online Mindful Self-Compassion Therapy on Sleep Quality and Pain Adaptation to in Employees with Physical Disabilities: A Quasi-Experimental Study. Prev Care Nurs Midwifery J 2026; 16 (2) :13-25
URL: http://nmcjournal.zums.ac.ir/article-1-1008-en.html
URL: http://nmcjournal.zums.ac.ir/article-1-1008-en.html



Department of Psychology and Educational Sciences, Faculty of Humanities, Khatam University, Tehran, Iran , a.khodabakhshid@khatam.ac.ir
Keywords: Self-compassion Therapy, Mindfulness, Sleep Quality, Adaptation to Chronic Pain, Physical Disability, Online Intervention
Full-Text [PDF 877 kb]
(75 Downloads)
| Abstract (HTML) (385 Views)
Full-Text: (45 Views)
Introduction
Disability encompasses a broad spectrum of physical, psychological, and cognitive conditions that can substantially affect individuals’ independence and daily functioning [1]. People with physical disabilities frequently face numerous challenges and require continuous support throughout their lives. Such support systems can serve as a protective buffer, reducing their level of dependency, enhancing their autonomy, and ultimately improving their overall quality of life [2].
Living with a permanent physical disability often results in dependence and difficulties in maintaining an active lifestyle. Consequently, individuals with physical disabilities tend to adopt sedentary patterns of living, which increases their risk of secondary health conditions and decreases their health-related physical fitness [3]. A meta-analysis has highlighted significant disparities in quality of life between individuals with physical disabilities and adults without such disabilities [4]. Addressing both physical and psychological dimensions is therefore essential for reducing these quality-of-life disparities, underscoring an urgent concern in public health [3].
Given the nature of their physical limitations and functional challenges, individuals with disabilities often fail to experience deep, restorative sleep [5]. Thus, sleep quality emerges as a crucial factor that can influence their quality of life and social participation. People with physical disabilities typically suffer from poor sleep quality due to mobility limitations, a condition that in turn contributes to heightened anxiety and depression [6]. Poor sleep quality leads to adverse consequences such as headaches, learning difficulties, memory impairment, behavioral aggression, and reduced cognitive functioning. Moreover, diminished sleep quality is associated with depression, anxiety, quality of life, and one’s ability to cope with everyday stressors [5].
Numerous studies have examined the association between pain and disability. Huang et al., for instance, found that pain intensity is linked to disability in patients with chronic low back pain [7]. Psychological aspects of pain and activity-limiting life restrictions are frequently reported among individuals with spinal cord injuries [8]. Chronic pain is one of the most prevalent issues among individuals with physical disabilities, exerting serious negative effects on their quality of life, daily functioning, and mental health [9]. Because chronic pain and sleep problems are influenced not only by physical limitations but also by self‑criticism, emotional distress, and heightened arousal, approaches that cultivate mindful self‑compassion may help improve both conditions.
Compassion-focused therapy (CFT) employs techniques such as self-acceptance, self-respect, the strengthening of self-confidence, and the cultivation of positive emotions to help individuals cope with destructive thoughts, depression, anxiety, and distressing feelings of shame and self-criticism. This therapeutic approach is widely applicable across clinical populations as well as individuals with physical health conditions [10]. Grounded in an evolutionary and neuropsychological framework of mental health problems, compassion-focused therapy has demonstrated substantial therapeutic effects [11]. Neff’s model conceptualizes self‑compassion as comprising self‑kindness, common humanity, and mindful awareness, which together reduce self‑criticism and maladaptive affective responses while enhancing adaptive regulation of distressing emotions. Higher self‑compassion is consistently associated with better emotion regulation, lower negative effects, and healthier coping behaviors, mechanisms believed to decrease psychological arousal and facilitate more restorative sleep [2-13]. The integration of these three interrelated components forms the basis of an individual’s compassionate relationship with themselves. Consequently, this conceptualization was widely incorporated by Gilbert into compassion-focused therapy [14]. Mindful self-compassion therapy, introduced by Gilbert and Choden [15] and inspired by Jon Kabat-Zinn’s mindfulness-based stress reduction (MBSR) program [16] merges both therapeutic traditions. This integrated framework can meaningfully support individuals with disabilities in recognizing and restoring their sense of independence [17].
Individuals with physical disabilities frequently experience chronic pain and sleep disturbances, which can substantially diminish quality of life and increase vulnerability to long-term health problems. Beyond physical limitations, the emotional burden associated with disability often contributes to lower levels of mindfulness and self-compassion, accompanied by feelings of insecurity, worthlessness, and psychological instability. Although mindfulness‑ and self‑compassion‑based interventions have been shown to be helpful in general and clinical populations, most studies have focused on in‑person programs or individuals without disabilities. As a result, there is still limited evidence on the effectiveness of online mindful self‑compassion interventions for people with physical disabilities, especially those who are employed.
To address this gap, the present study introduces an innovative online mindful self-compassion intervention designed to overcome access barriers and promote inclusivity. Emerging evidence indicates that online psychological interventions can be effective, scalable, and acceptable, while reducing logistical and physical constraints associated with face-to-face delivery. From a preventive care perspective, interventions that improve sleep quality and enhance adaptive responses to chronic pain may help prevent secondary physical and psychological complications, strengthen emotional resilience, and support overall wellbeing.
Objectives
The present study aimed to evaluate the effectiveness of online mindful self-compassion therapy on sleep quality and exploratorily examine its effects on pain adaptation among employees with physical disabilities.
Methods
Study Design
This quasi‑experimental study was conducted with a pretest- posttest design and a control group in from August 2025 to December 2025.
Participants & Sampling
The National Iranian Gas Company employs approximately 80,000 individuals, of whom 1,100 were identified as employees with physical disabilities.
Due to the exploratory nature of this study and the absence of prior effect size estimates for online mindful self‑compassion interventions in this specific population, a convenience sampling method was employed. Thirty eligible participants were recruited through internal company communications (email and notice boards). After the study requirements were explained, these 30 individuals were non‑randomly assigned to the experimental group (n = 15) or wait‑list control group (n = 15) based on their order of enrollment and matching for key demographic variables (age, gender, and education). True randomization was not performed, and the study was not registered in the IRCT, consistent with its quasi‑experimental design.
A total of 1,100 employees with physical disabilities working at the National Iranian Gas Company were identified as the accessible population. Of these, 187 individuals responded to the internal company announcement (email and notice boards) and expressed initial interest in participating. After initial telephone screening to assess basic eligibility (age range 30–48 years, self-reported sleep disturbances or chronic pain, and access to stable internet connection), 52 individuals met the preliminary inclusion criteria and were invited for a full in-person or online eligibility interview. Following the complete eligibility assessment based on medical and social welfare records verification, 22 individuals were excluded for the following reasons: severe cognitive or psychiatric conditions interfering with participation (n = 10), concurrent participation in other structured psychological or pain‑management interventions (n = 8), and unstable dosage of sedative or analgesic medications (n = 4). Thus, 30 eligible participants were initially enrolled and provided informed consent (Diagram 1). A final sample of 30 participants (15 in the experimental group, 15 in the control group) completed all pre‑test and post‑test assessments and were included in the final analysis. No participants were excluded from the analysis due to missing data, as all 30 completers provided full data.
Sample Size Justification and Post‑Hoc Power Analysis
Although a priori power analysis could not be conducted due to the lack of pilot data in this population, a post‑hoc power analysis was performed using G*Power 3.1.9.7 [18] to inform future research and to interpret the null findings appropriately. Based on the observed effect sizes in this study:
Disability encompasses a broad spectrum of physical, psychological, and cognitive conditions that can substantially affect individuals’ independence and daily functioning [1]. People with physical disabilities frequently face numerous challenges and require continuous support throughout their lives. Such support systems can serve as a protective buffer, reducing their level of dependency, enhancing their autonomy, and ultimately improving their overall quality of life [2].
Living with a permanent physical disability often results in dependence and difficulties in maintaining an active lifestyle. Consequently, individuals with physical disabilities tend to adopt sedentary patterns of living, which increases their risk of secondary health conditions and decreases their health-related physical fitness [3]. A meta-analysis has highlighted significant disparities in quality of life between individuals with physical disabilities and adults without such disabilities [4]. Addressing both physical and psychological dimensions is therefore essential for reducing these quality-of-life disparities, underscoring an urgent concern in public health [3].
Given the nature of their physical limitations and functional challenges, individuals with disabilities often fail to experience deep, restorative sleep [5]. Thus, sleep quality emerges as a crucial factor that can influence their quality of life and social participation. People with physical disabilities typically suffer from poor sleep quality due to mobility limitations, a condition that in turn contributes to heightened anxiety and depression [6]. Poor sleep quality leads to adverse consequences such as headaches, learning difficulties, memory impairment, behavioral aggression, and reduced cognitive functioning. Moreover, diminished sleep quality is associated with depression, anxiety, quality of life, and one’s ability to cope with everyday stressors [5].
Numerous studies have examined the association between pain and disability. Huang et al., for instance, found that pain intensity is linked to disability in patients with chronic low back pain [7]. Psychological aspects of pain and activity-limiting life restrictions are frequently reported among individuals with spinal cord injuries [8]. Chronic pain is one of the most prevalent issues among individuals with physical disabilities, exerting serious negative effects on their quality of life, daily functioning, and mental health [9]. Because chronic pain and sleep problems are influenced not only by physical limitations but also by self‑criticism, emotional distress, and heightened arousal, approaches that cultivate mindful self‑compassion may help improve both conditions.
Compassion-focused therapy (CFT) employs techniques such as self-acceptance, self-respect, the strengthening of self-confidence, and the cultivation of positive emotions to help individuals cope with destructive thoughts, depression, anxiety, and distressing feelings of shame and self-criticism. This therapeutic approach is widely applicable across clinical populations as well as individuals with physical health conditions [10]. Grounded in an evolutionary and neuropsychological framework of mental health problems, compassion-focused therapy has demonstrated substantial therapeutic effects [11]. Neff’s model conceptualizes self‑compassion as comprising self‑kindness, common humanity, and mindful awareness, which together reduce self‑criticism and maladaptive affective responses while enhancing adaptive regulation of distressing emotions. Higher self‑compassion is consistently associated with better emotion regulation, lower negative effects, and healthier coping behaviors, mechanisms believed to decrease psychological arousal and facilitate more restorative sleep [2-13]. The integration of these three interrelated components forms the basis of an individual’s compassionate relationship with themselves. Consequently, this conceptualization was widely incorporated by Gilbert into compassion-focused therapy [14]. Mindful self-compassion therapy, introduced by Gilbert and Choden [15] and inspired by Jon Kabat-Zinn’s mindfulness-based stress reduction (MBSR) program [16] merges both therapeutic traditions. This integrated framework can meaningfully support individuals with disabilities in recognizing and restoring their sense of independence [17].
Individuals with physical disabilities frequently experience chronic pain and sleep disturbances, which can substantially diminish quality of life and increase vulnerability to long-term health problems. Beyond physical limitations, the emotional burden associated with disability often contributes to lower levels of mindfulness and self-compassion, accompanied by feelings of insecurity, worthlessness, and psychological instability. Although mindfulness‑ and self‑compassion‑based interventions have been shown to be helpful in general and clinical populations, most studies have focused on in‑person programs or individuals without disabilities. As a result, there is still limited evidence on the effectiveness of online mindful self‑compassion interventions for people with physical disabilities, especially those who are employed.
To address this gap, the present study introduces an innovative online mindful self-compassion intervention designed to overcome access barriers and promote inclusivity. Emerging evidence indicates that online psychological interventions can be effective, scalable, and acceptable, while reducing logistical and physical constraints associated with face-to-face delivery. From a preventive care perspective, interventions that improve sleep quality and enhance adaptive responses to chronic pain may help prevent secondary physical and psychological complications, strengthen emotional resilience, and support overall wellbeing.
Objectives
The present study aimed to evaluate the effectiveness of online mindful self-compassion therapy on sleep quality and exploratorily examine its effects on pain adaptation among employees with physical disabilities.
Methods
Study Design
This quasi‑experimental study was conducted with a pretest- posttest design and a control group in from August 2025 to December 2025.
Participants & Sampling
The National Iranian Gas Company employs approximately 80,000 individuals, of whom 1,100 were identified as employees with physical disabilities.
Due to the exploratory nature of this study and the absence of prior effect size estimates for online mindful self‑compassion interventions in this specific population, a convenience sampling method was employed. Thirty eligible participants were recruited through internal company communications (email and notice boards). After the study requirements were explained, these 30 individuals were non‑randomly assigned to the experimental group (n = 15) or wait‑list control group (n = 15) based on their order of enrollment and matching for key demographic variables (age, gender, and education). True randomization was not performed, and the study was not registered in the IRCT, consistent with its quasi‑experimental design.
A total of 1,100 employees with physical disabilities working at the National Iranian Gas Company were identified as the accessible population. Of these, 187 individuals responded to the internal company announcement (email and notice boards) and expressed initial interest in participating. After initial telephone screening to assess basic eligibility (age range 30–48 years, self-reported sleep disturbances or chronic pain, and access to stable internet connection), 52 individuals met the preliminary inclusion criteria and were invited for a full in-person or online eligibility interview. Following the complete eligibility assessment based on medical and social welfare records verification, 22 individuals were excluded for the following reasons: severe cognitive or psychiatric conditions interfering with participation (n = 10), concurrent participation in other structured psychological or pain‑management interventions (n = 8), and unstable dosage of sedative or analgesic medications (n = 4). Thus, 30 eligible participants were initially enrolled and provided informed consent (Diagram 1). A final sample of 30 participants (15 in the experimental group, 15 in the control group) completed all pre‑test and post‑test assessments and were included in the final analysis. No participants were excluded from the analysis due to missing data, as all 30 completers provided full data.
Sample Size Justification and Post‑Hoc Power Analysis
Although a priori power analysis could not be conducted due to the lack of pilot data in this population, a post‑hoc power analysis was performed using G*Power 3.1.9.7 [18] to inform future research and to interpret the null findings appropriately. Based on the observed effect sizes in this study:
- For sleep quality (η² = 0.204, equivalent to f² = 0.256), a total sample of 42 participants (21 per group) would be required to achieve 80% power with α = 0.05, two groups, and one covariate.
- For pain adaptation (η² = 0.079, equivalent to f² = 0.086, a medium effect), a total sample of 118 participants (59 per group) would be required under the same conditions.
Thus, the present sample of 30 participants was severely underpowered for detecting effects on pain adaptation (achieved power = 0.29). This limitation is critical and means that any non‑significant finding for pain adaptation cannot be interpreted as evidence of no effect; rather, it reflects the study's insufficient sample size.
Inclusion and Exclusion Criteria
Participants were employees of the National Iranian Gas Company with a documented physical disability verified by medical and social welfare records, aged 30–48 years, experiencing sleep disturbances or chronic pain based on self-report or initial screening, and ability to participate in online sessions with access to a stable internet connection.
Individuals were excluded if they had severe cognitive, psychiatric, or neurological conditions (confirmed through medical records) that could interfere with participation, were concurrently receiving other structured psychological or pain-management interventions, or were using sedative, hypnotic, or analgesic medications affecting sleep or pain unless the dosage had been stable for at least one month prior to enrollment.
Interventions
The intervention program was designed using material from the book Mindful Compassion [14] and delivered in alignment with its principles. A concise overview of the program’s content is presented in Table 1.
Eight online compassion-focused therapy sessions were conducted online in a virtual environment.
Comparison
In this study, a call for participation was announced via internal company communications, including email and notice boards, inviting employees with documented physical disabilities to volunteer. Among responders, 30 individuals were selected after the study requirements were explained either via telephone or in person.Participants were non‑randomly assigned to the intervention (n = 15) and control (n = 15) groups based on their order of enrollment. . Baseline assessments of sleep quality, pain adaptation, and self-compassion were completed online for all participants.
The experimental group participated in an 8-week online Mindful Self-Compassion program, consisting of weekly 40-minute live sessions that included exercises directed toward the self and others, meditation, and related mindfulness techniques. Sessions were scheduled at times convenient for participants and coordinated via the Gharar platform (https://gharar.ir/), which provided interactive features such as live chat, polls, and breakout rooms to enhance engagement and discussion. Prior to enrollment, participants’ access and ability to log in were verified. To ensure protocol adherence, all sessions were guided by a senior rehabilitation counseling specialist and monitored using a structured checklist. Instructional materials included PowerPoint presentations, brief educational videos, Persian-translated or subtitled clips, and mindfulness-based relaxation exercises.
During the intervention period, the control group did not receive any structured intervention; no educational materials were provided. No direct contact occurred between the two groups, and access restrictions and individual logins minimized the risk of sharing intervention materials. After completion of post-test assessments in the intervention group, the control group received the same eight online sessions to address ethical considerations.
Following the intervention, post-test assessments were conducted to examine changes in sleep quality, pain adaptation, and self-compassion. Participant engagement, session adherence, and completion were carefully monitored to maintain intervention fidelity and minimize attrition. This design ensured a controlled comparison while accommodating the specific accessibility needs of employees with physical disabilities. Both groups completed assessments of sleep quality and pain adaptation at baseline and after the intervention. Participant engagement and completion were monitored throughout the study, and attrition was minimal, ensuring the integrity of the collected data.
Outcomes
The study measured changes in sleep quality and adaptation to chronic pain to evaluate the effect of the intervention. Pre-test and post-test assessments were conducted using the Pittsburgh Sleep Quality Index (PSQI) and the Adaptation to Chronic Pain Questionnaire (ACPQ). For this study, the primary outcomes were operationally defined as follows:
Inclusion and Exclusion Criteria
Participants were employees of the National Iranian Gas Company with a documented physical disability verified by medical and social welfare records, aged 30–48 years, experiencing sleep disturbances or chronic pain based on self-report or initial screening, and ability to participate in online sessions with access to a stable internet connection.
Individuals were excluded if they had severe cognitive, psychiatric, or neurological conditions (confirmed through medical records) that could interfere with participation, were concurrently receiving other structured psychological or pain-management interventions, or were using sedative, hypnotic, or analgesic medications affecting sleep or pain unless the dosage had been stable for at least one month prior to enrollment.
Interventions
The intervention program was designed using material from the book Mindful Compassion [14] and delivered in alignment with its principles. A concise overview of the program’s content is presented in Table 1.
Eight online compassion-focused therapy sessions were conducted online in a virtual environment.
Comparison
In this study, a call for participation was announced via internal company communications, including email and notice boards, inviting employees with documented physical disabilities to volunteer. Among responders, 30 individuals were selected after the study requirements were explained either via telephone or in person.Participants were non‑randomly assigned to the intervention (n = 15) and control (n = 15) groups based on their order of enrollment. . Baseline assessments of sleep quality, pain adaptation, and self-compassion were completed online for all participants.
The experimental group participated in an 8-week online Mindful Self-Compassion program, consisting of weekly 40-minute live sessions that included exercises directed toward the self and others, meditation, and related mindfulness techniques. Sessions were scheduled at times convenient for participants and coordinated via the Gharar platform (https://gharar.ir/), which provided interactive features such as live chat, polls, and breakout rooms to enhance engagement and discussion. Prior to enrollment, participants’ access and ability to log in were verified. To ensure protocol adherence, all sessions were guided by a senior rehabilitation counseling specialist and monitored using a structured checklist. Instructional materials included PowerPoint presentations, brief educational videos, Persian-translated or subtitled clips, and mindfulness-based relaxation exercises.
During the intervention period, the control group did not receive any structured intervention; no educational materials were provided. No direct contact occurred between the two groups, and access restrictions and individual logins minimized the risk of sharing intervention materials. After completion of post-test assessments in the intervention group, the control group received the same eight online sessions to address ethical considerations.
Following the intervention, post-test assessments were conducted to examine changes in sleep quality, pain adaptation, and self-compassion. Participant engagement, session adherence, and completion were carefully monitored to maintain intervention fidelity and minimize attrition. This design ensured a controlled comparison while accommodating the specific accessibility needs of employees with physical disabilities. Both groups completed assessments of sleep quality and pain adaptation at baseline and after the intervention. Participant engagement and completion were monitored throughout the study, and attrition was minimal, ensuring the integrity of the collected data.
Outcomes
The study measured changes in sleep quality and adaptation to chronic pain to evaluate the effect of the intervention. Pre-test and post-test assessments were conducted using the Pittsburgh Sleep Quality Index (PSQI) and the Adaptation to Chronic Pain Questionnaire (ACPQ). For this study, the primary outcomes were operationally defined as follows:
- Improved sleep quality: a reduction in the total PSQI score from pre-test to post-test, with lower scores indicating better subjective sleep quality, shorter sleep latency, longer sleep duration, and improved sleep efficiency.
- Enhanced adaptation to chronic pain: an increase in the total ACPQ score from pre-test to post-test, reflecting improved coping strategies, functional adjustment, and acceptance of chronic pain.
These operational definitions allowed for quantitative evaluation of intervention effects and facilitated comparison between the intervention and control groups.
Data Collection
The data were collected using the Demographic Information Checklist, Pittsburgh Sleep Quality Index (PSQI), and the Adaptation to Chronic Pain Questionnaire.
Demographic and background information collected from participants included age (in years), gender (male or female), and educational level (categorized as high school, diploma, bachelor’s, master’s, or PhD).
Pittsburgh Sleep Quality Index (PSQI): The PSQI was originally developed and validated by Buysse et al. This self-report instrument contains 19 items distributed across seven components assessing various aspects of sleep, including subjective sleep quality, sleep latency, sleep duration and efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction resulting from insufficient sleep. Each component is rated on a scale from 0 to 3, producing a total score ranging from 0 to 21, where higher scores indicate poorer sleep quality. A total score above 5 signifies the presence of sleep disturbances [19]. The Persian version of the Pittsburgh Sleep Quality Index (PSQI-P) has demonstrated acceptable validity and reliability in previous studies. Farrahi Moghaddam et al. reported good internal consistency for the PSQI-P, with a Cronbach’s alpha coefficient of 0.77, and confirmed its construct validity in an Iranian population [20]. For the present study, the reliability of the instrument was reassessed in the population of individuals with physical disabilities, yielding a Cronbach’s alpha coefficient of 0.85.
Adaptation to Chronic Pain Questionnaire (ACPQ): Developed by Zavadilova and Knotek, this questionnaire is rooted in health psychology and assesses cognitive-emotional responses to chronic pain. It consists of 18 items scored on a four-point Likert scale ranging from “strongly agree” to “strongly disagree,” with lower scores reflecting greater adaptation to pain. The instrument encompasses three conceptual dimensions that are embedded throughout its items: the individual’s perception of personal abilities and roles (self-perception), their acceptance of pain-related limitations (perceived limitations), and their perceived capacity to manage and withstand pain (perceived tolerance) [21]. The reliability and validity of the Persian version of the Adaptation to Chronic Pain Questionnaire were evaluated by Hosseininia et al. The authors assessed internal consistency and reported acceptable reliability for the total scale and its subscales. Construct validity was examined using factor analysis, which supported the underlying factor structure of the Persian version. In addition, convergent validity was confirmed through significant correlations with related psychological constructs. Overall, the findings indicate that the Persian version of the Adaptation to Chronic Pain Questionnaire possesses satisfactory psychometric properties and is a valid and reliable instrument for use in Iranian populations [22]. In this study, the Persian version of the questionnaire was used and administered to individuals with physical disabilities. The reliability of the instrument was confirmed in the present sample, yielding a Cronbach’s alpha coefficient of 0.91.
Statistical Analysis
All analyses were performed using SPSS (Version 25). Descriptive statistics are presented as mean (SD) for continuous variables and as frequency (percentage) for categorical variables.
The normality of data was examined using the Shapiro–Wilk test, and homogeneity of variances/covariances was assessed via Levene’s test and Box’s M test. To test the primary hypotheses, a multivariate analysis of covariance (MANCOVA) was first conducted with the three primary outcome measures (sleep quality, pain adaptation, self-compassion) as dependent variables, group (intervention vs. control) as the independent variable, and pre-test scores as covariates. This assessed the overall intervention effect across all outcomes. Where the MANCOVA yielded a significant omnibus effect, separate one-way analyses of covariance (ANCOVAs) were then performed for each outcome to identify specific effects, again controlling pre-test scores. The assumption of homogeneity of regression slopes was verified for each ANCOVA.
For significant ANCOVA results, post-hoc pairwise comparisons were conducted using the Bonferroni correction to control for Type I error. Statistical significance was set at p < 0.05 (two-tailed). Effect sizes are reported as partial eta squared (ηp²), with values of 0.01, 0.06, and 0.14 interpreted as small, medium, and large, respectively. All analytical plans were pre-specified to ensure transparency.
Result
Table 2 presents the demographic characteristics of the final sample of 30 participants. The gender composition was relatively balanced, with approximately 60% male and 40% female participants. The mean age of the participants was 38.4 years (SD = 5.2), ranging from 30 to 48 years, indicating a relatively homogeneous sample group. Moreover, most participants held a university-level education (bachelor's degree or higher).
As presented in Table 3, at pre-test, the experimental and control groups had comparable scores on sleep quality (experimental: M = 19.18, SD = 3.50; control: M = 19.01, SD = 4.51) and pain adaptation (experimental: M = 46.20, SD = 12.83; control: M = 49.93, SD = 12.82), indicating no initial differences between the groups.
Following the intervention, the experimental group demonstrated a notable improvement in sleep quality, with mean scores decreasing to 14.56 (SD = 6.27), whereas the control group showed a slight increase to 20.14 (SD = 4.39). In contrast, changes in pain adaptation were minimal in both groups, with the experimental group slightly decreasing to 45.20 (SD = 7.71) and the control group slightly increasing to 50.86 (SD = 11.11).
Prior to conducting MANCOVA, all assumptions were examined and satisfied. Normality was confirmed using the Shapiro–Wilk test (p > .05), homogeneity of variance–covariance matrices by Box's M test (p > 0.05), equality of error variances by Levene's test (p > 0.05), and homogeneity of regression slopes by testing the interaction between the covariate and the independent variable (p > 0.05).
The results of MANCOVA (see Table 4) indicated a significant overall effect of the intervention on the combined dependent variables. The multivariate tests yielded the following values: Pillai's Trace = 0.42, F = 5.59, p < .05; Wilks' Lambda = 0.57, F = 5.58, p < .05; Hotelling's Trace = 0.72, F = 5.60, p < .05; Roy's Largest Root = 0.73, F = 5.61, p < .05. This indicates that, after controlling for pre-test differences, the intervention significantly influenced the linear combination of sleep quality and pain adaptation scores. As shown in Table 4, further univariate analyses revealed that the intervention had a statistically significant effect on sleep quality (F = 6.39, p = .012, η² = 0.204, large effect size, power = 0.68). For pain adaptation (Table 4), the analysis yielded a non‑statistically significant result (F = 2.13, p = .151, η² = 0.079, medium effect size, power = 0.29). Given the power of 0.29 (well below the conventional threshold of 0.80), this null finding is inconclusive. Specifically, the study had only a 29% chance of detecting the observed medium effect if it truly exists in the population. Therefore, this result should not be interpreted as evidence that the intervention does not improve pain adaptation, but rather as an indication that the study was insufficiently powered to evaluate this outcome.
Data Collection
The data were collected using the Demographic Information Checklist, Pittsburgh Sleep Quality Index (PSQI), and the Adaptation to Chronic Pain Questionnaire.
Demographic and background information collected from participants included age (in years), gender (male or female), and educational level (categorized as high school, diploma, bachelor’s, master’s, or PhD).
Pittsburgh Sleep Quality Index (PSQI): The PSQI was originally developed and validated by Buysse et al. This self-report instrument contains 19 items distributed across seven components assessing various aspects of sleep, including subjective sleep quality, sleep latency, sleep duration and efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction resulting from insufficient sleep. Each component is rated on a scale from 0 to 3, producing a total score ranging from 0 to 21, where higher scores indicate poorer sleep quality. A total score above 5 signifies the presence of sleep disturbances [19]. The Persian version of the Pittsburgh Sleep Quality Index (PSQI-P) has demonstrated acceptable validity and reliability in previous studies. Farrahi Moghaddam et al. reported good internal consistency for the PSQI-P, with a Cronbach’s alpha coefficient of 0.77, and confirmed its construct validity in an Iranian population [20]. For the present study, the reliability of the instrument was reassessed in the population of individuals with physical disabilities, yielding a Cronbach’s alpha coefficient of 0.85.
Adaptation to Chronic Pain Questionnaire (ACPQ): Developed by Zavadilova and Knotek, this questionnaire is rooted in health psychology and assesses cognitive-emotional responses to chronic pain. It consists of 18 items scored on a four-point Likert scale ranging from “strongly agree” to “strongly disagree,” with lower scores reflecting greater adaptation to pain. The instrument encompasses three conceptual dimensions that are embedded throughout its items: the individual’s perception of personal abilities and roles (self-perception), their acceptance of pain-related limitations (perceived limitations), and their perceived capacity to manage and withstand pain (perceived tolerance) [21]. The reliability and validity of the Persian version of the Adaptation to Chronic Pain Questionnaire were evaluated by Hosseininia et al. The authors assessed internal consistency and reported acceptable reliability for the total scale and its subscales. Construct validity was examined using factor analysis, which supported the underlying factor structure of the Persian version. In addition, convergent validity was confirmed through significant correlations with related psychological constructs. Overall, the findings indicate that the Persian version of the Adaptation to Chronic Pain Questionnaire possesses satisfactory psychometric properties and is a valid and reliable instrument for use in Iranian populations [22]. In this study, the Persian version of the questionnaire was used and administered to individuals with physical disabilities. The reliability of the instrument was confirmed in the present sample, yielding a Cronbach’s alpha coefficient of 0.91.
Statistical Analysis
All analyses were performed using SPSS (Version 25). Descriptive statistics are presented as mean (SD) for continuous variables and as frequency (percentage) for categorical variables.
The normality of data was examined using the Shapiro–Wilk test, and homogeneity of variances/covariances was assessed via Levene’s test and Box’s M test. To test the primary hypotheses, a multivariate analysis of covariance (MANCOVA) was first conducted with the three primary outcome measures (sleep quality, pain adaptation, self-compassion) as dependent variables, group (intervention vs. control) as the independent variable, and pre-test scores as covariates. This assessed the overall intervention effect across all outcomes. Where the MANCOVA yielded a significant omnibus effect, separate one-way analyses of covariance (ANCOVAs) were then performed for each outcome to identify specific effects, again controlling pre-test scores. The assumption of homogeneity of regression slopes was verified for each ANCOVA.
For significant ANCOVA results, post-hoc pairwise comparisons were conducted using the Bonferroni correction to control for Type I error. Statistical significance was set at p < 0.05 (two-tailed). Effect sizes are reported as partial eta squared (ηp²), with values of 0.01, 0.06, and 0.14 interpreted as small, medium, and large, respectively. All analytical plans were pre-specified to ensure transparency.
Result
Table 2 presents the demographic characteristics of the final sample of 30 participants. The gender composition was relatively balanced, with approximately 60% male and 40% female participants. The mean age of the participants was 38.4 years (SD = 5.2), ranging from 30 to 48 years, indicating a relatively homogeneous sample group. Moreover, most participants held a university-level education (bachelor's degree or higher).
As presented in Table 3, at pre-test, the experimental and control groups had comparable scores on sleep quality (experimental: M = 19.18, SD = 3.50; control: M = 19.01, SD = 4.51) and pain adaptation (experimental: M = 46.20, SD = 12.83; control: M = 49.93, SD = 12.82), indicating no initial differences between the groups.
Following the intervention, the experimental group demonstrated a notable improvement in sleep quality, with mean scores decreasing to 14.56 (SD = 6.27), whereas the control group showed a slight increase to 20.14 (SD = 4.39). In contrast, changes in pain adaptation were minimal in both groups, with the experimental group slightly decreasing to 45.20 (SD = 7.71) and the control group slightly increasing to 50.86 (SD = 11.11).
Prior to conducting MANCOVA, all assumptions were examined and satisfied. Normality was confirmed using the Shapiro–Wilk test (p > .05), homogeneity of variance–covariance matrices by Box's M test (p > 0.05), equality of error variances by Levene's test (p > 0.05), and homogeneity of regression slopes by testing the interaction between the covariate and the independent variable (p > 0.05).
The results of MANCOVA (see Table 4) indicated a significant overall effect of the intervention on the combined dependent variables. The multivariate tests yielded the following values: Pillai's Trace = 0.42, F = 5.59, p < .05; Wilks' Lambda = 0.57, F = 5.58, p < .05; Hotelling's Trace = 0.72, F = 5.60, p < .05; Roy's Largest Root = 0.73, F = 5.61, p < .05. This indicates that, after controlling for pre-test differences, the intervention significantly influenced the linear combination of sleep quality and pain adaptation scores. As shown in Table 4, further univariate analyses revealed that the intervention had a statistically significant effect on sleep quality (F = 6.39, p = .012, η² = 0.204, large effect size, power = 0.68). For pain adaptation (Table 4), the analysis yielded a non‑statistically significant result (F = 2.13, p = .151, η² = 0.079, medium effect size, power = 0.29). Given the power of 0.29 (well below the conventional threshold of 0.80), this null finding is inconclusive. Specifically, the study had only a 29% chance of detecting the observed medium effect if it truly exists in the population. Therefore, this result should not be interpreted as evidence that the intervention does not improve pain adaptation, but rather as an indication that the study was insufficiently powered to evaluate this outcome.
| Session | Objectives and Topics |
Exercises and materials | Supporting tools and homework |
| 1 | Introduction of participants; establishing rules and signing the training agreement; explanation of basic concepts | Group discussion; pre-test questionnaire | Self-help booklet; Self-Compassion Questionnaire |
| 2 | Training in mindfulness and identifying the inner critical voice | Diaphragmatic breathing exercise; recording self-critical thoughts | Guided audio files; thought-recording worksheets |
| 3 | Safe imagery and cultivating a sense of security | “Safe place” imagery exercise | Guided imagery audio file |
| 4 | Introduction to self-compassion and differentiation from self-judgment | Writing a compassionate letter to oneself | Standard sample letters |
| 5 | Application of compassion in dealing with failure and shame | Role-playing challenging situations using a compassion-focused approach | Practice scenarios |
| 6 | Strengthening compassion-based behaviors in daily life | Setting small compassion-focused goals (e.g., being kind to oneself during stress) | Behavioral follow-up checklist |
| 7 | Integration of learned skills and addressing remaining barriers | Feedback and troubleshooting | Post-test questionnaire |
| 8 | Summary, obtaining final feedback, future planning, and closure | Developing a personalized plan for the continuation of practice |
| Characteristic | Level | Total (N = 30) | Experimental (n = 15) | Control (n = 15) | p |
| Gender, n (%) | Male | 18 (60%) | 9 (60%) | 9 (60%) | .291 |
| Female | 12 (40%) | 6 (40%) | 6 (40%) | ||
| Age (years), M (SD) | 38.4 (5.2) | 38.1 (5.4) | 38.7 (5.1) | .312 | |
| Education, n (%) | Diploma or below | 6 (20%) | 3 (20%) | 3 (20%) | .521 |
| Bachelor's degree | 16 (53%) | 8 (53%) | 8 (53%) | ||
| Master's degree or above | 8 (27%) | 4 (27%) | 4 (27%) |
P-values were calculated using the chi-square test for categorical variables and independent t-test for age. Percentages may not total 100 due to rounding.
Table 3. Descriptive Statistics for Sleep Quality and Pain Adaptation at Pre-test and Post-test
| Variable | Time | Group | n | M | SD | Min | Max |
| Sleep Quality | Pre-test | Experimental | 15 | 19.18 | 3.50 | 13.00 | 26.00 |
| Control | 15 | 19.01 | 4.51 | 12.00 | 28.00 | ||
| Post-test | Experimental | 15 | 14.56 | 6.27 | 10.00 | 29.00 | |
| Control | 15 | 20.14 | 4.39 | 13.00 | 30.00 | ||
| Pain Adaptation | Pre-test | Experimental | 15 | 46.20 | 12.83 | 34.00 | 71.00 |
| Control | 15 | 49.93 | 12.82 | 23.00 | 70.00 | ||
| Post-test | Experimental | 15 | 45.20 | 7.71 | 29.00 | 54.00 | |
| Control | 15 | 50.86 | 11.11 | 32.00 | 70.00 |
M = mean; SD = standard deviation; Min = minimum; Max = maximum.
Table 4. Multivariate and Univariate Results of MANCOVA for the Effect of Online Mindful Self-Compassion Intervention on Sleep Quality and Pain Adaptation
Table 4. Multivariate and Univariate Results of MANCOVA for the Effect of Online Mindful Self-Compassion Intervention on Sleep Quality and Pain Adaptation
| Outcome | Source | Test / Effect | Value | F | df | p | η² | Effect Size Interpretation | Power |
| Multivariate (combined) | Intervention | Pillai's Trace | 0.42 | 5.59 | - | < .05 | 0.42 | Large | - |
| Wilks' Lambda | 0.57 | 5.58 | - | < .05 | 0.57 | Large | - | ||
| Hotelling's Trace | 0.72 | 5.60 | - | < .05 | 0.72 | Large | - | ||
| Roy's Largest Root | 0.73 | 5.61 | - | < .05 | 0.73 | Large | - | ||
| Sleep Quality | Intervention | Univariate ANCOVA | - | 6.39 | 1, 25 | .012 | 0.204 | Large | 0.68 |
| Pain Adaptation | Intervention | Univariate ANCOVA | - | 2.13 | 1, 25 | .151 | 0.079 | Medium | 0.29 |
df = degrees of freedom; η² = partial eta squared. Pre-test scores were used as covariates. Effect size interpretation based on conventional benchmarks (small = 0.01, medium = 0.06, large = 0.14).
Discussion
The present study examined the effectiveness of an online Mindful Self-Compassion program on sleep quality and pain adaptation among physically disabled employees of the National Iranian Gas Company. Individuals with physical disabilities often experience complex challenges such as chronic pain, sleep disturbances, and reduced quality of life, which negatively impact mental health, social functioning, and occupational performance. Addressing these issues through psychological interventions that foster emotional resilience, self-regulation, and self-compassion have become increasingly important.
Effect of the Intervention on Sleep Quality
The results indicated that participation in the Mindful Self-Compassion intervention led to significant improvements in sleep quality, including fewer nocturnal awakenings, reduced sleep difficulties, and greater overall sleep satisfaction. These outcomes align with prior research demonstrating that self-compassion exercises reduce rumination, anxiety, and depression, thereby enhancing overall mental health and well-being.
In line with these findings, it can be argued that the core of compassion-focused therapy lies in self-compassion, care, understanding, and empathy. For a patient, self-compassion involves adopting a positive attitude toward one's current condition, particularly in the presence of uncontrollable chronic illness [23]. One study demonstrated that mindful compassion reduces pain catastrophizing and lowers rumination levels among women with mobility impairments [24]. Other studies have demonstrated, based on the self-regulation behavior model, that self-compassion can promote healthy behaviors, such as sleep, by fostering adaptive emotional states [25]. Specifically, self-compassion has the potential to act as a protective factor for emotional regulation and coping capacities, thereby safeguarding sleep quality [26]. Previous studies have also shown that positive thoughts and self-kindness are adaptive emotions that enhance healthy behaviors and protect sleep quality [25]. Findings suggest that individuals exhibiting higher levels of self-compassion are more likely to adopt positive coping strategies in response to stress [27], potentially because they are more attentive and responsive to their own emotions and needs [26].
Mindfulness plays a key role in this process by cultivating present-moment, nonjudgmental awareness of negative thoughts and emotions, thereby reducing pre-sleep activation of the nervous system. This mechanism is particularly important for individuals with physical disabilities who face stress, worry, and feelings of inefficacy, as it can help increase pre-sleep relaxation and overall sleep quality [14-16]. Research has shown that increasing self-compassion facilitates the mental pathway to sleep by enhancing internal security and reducing self-criticism. Hence, delivering this intervention online not only provides easier accessibility and cost-effectiveness but can also effectively improve sleep quality in individuals with disabilities, ultimately contributing to the psychological and physical well-being of these individuals [17,24].
Effect of the Intervention on Pain Adaptation
In contrast to the findings for sleep quality, no statistically significant effect was observed on adaptation to chronic pain (F = 2.13, p = .151, η² = 0.079). However, this finding must be interpreted very carefully. The observed effect size for pain adaptation was medium (η² = 0.079), but the statistical power was only 0.29, which is far below the recommended minimum of 0.80. This means that even if the intervention had a true medium-sized effect on pain adaptation in the population, this study had only a 29% chance of detecting it as statistically significant. Therefore, the non-significant result is highly likely to be a false negative (Type II error) and should not be taken as evidence that the intervention is ineffective for pain adaptation [29].
The most parsimonious conclusion is that the present study was severely underpowered for this outcome, rendering the p-value uninformative. Post-hoc power analysis indicated that a sample of 118 participants would be required to reliably detect the observed medium effect size. Future studies with adequate sample sizes (approximately 118 participants) are necessary to determine whether online mindful self-compassion therapy truly has no effect on pain adaptation or whether the effect could not be detected here due to insufficient statistical power [18].
Several factors could be considered for future research, but should not be overinterpreted given the primary limitation of low power. First, the Adaptation to Chronic Pain Questionnaire (ACPQ) may lack sensitivity to detect subtle changes in cognitive or emotional coping mechanisms over a short period. Second, the 8-week intervention duration may have been insufficient to modify deeply ingrained cognitions and emotional responses related to chronic pain. Third, the session content, while focused on general mindfulness and self-compassion, may not have been specifically tailored to target pain-related beliefs, coping strategies, or functional adaptation.
Consistent with the need for caution in interpreting null findings, previous studies that reported significant effects of compassion-focused therapy on pain-related outcomes typically had larger sample sizes and longer intervention durations. Psychologically, it shifts individuals' mindset from a "doing mode" to a "being mode" (28). However, these effects may require longer training periods or more pain-specific content than the present 8-week general mindful self-compassion program provided. For example, Mohamadpour [23] demonstrated that compassion-based therapy reduced pain catastrophizing in patients with multiple sclerosis, while Lanzaro et al [29] in their systematic review concluded that studies with sample sizes below 50 participants were consistently underpowered to detect effects on chronic pain outcomes. Similarly, Dou et al [30] found that mindfulness-based interventions required minimum sample sizes of 40–60 participants to detect significant effects on psychological outcomes in clinical populations.
Physiological studies have demonstrated that mindfulness training can reduce pain by altering anterior cingulate and insular cortex activity, alleviate emotional exhaustion, and reduce occupational burnout among nurses [30].
Consistent with the findings of this study, research has shown that compassion-focused therapy, originally developed to reduce high levels of shame and self-criticism, is grounded in evolutionary, social, and neurobiological understandings of human emotions [31]. Compassion-focused therapy aims to activate the soothing and affiliative emotion-regulation system, which is often underdeveloped in individuals with a history of trauma or chronic psychological pain. Integrating compassion-focused therapy with mindfulness, by cultivating self-kindness, emotional courage, and the capacity for compassionate engagement with suffering, further enriches the therapeutic approach [22,32]. Patients with spinal cord injury often struggle with identity disruption, loss of bodily control, and existential fears. Accordingly, Mindful Self-Compassion therapy provides a synergistic framework for restoring psychological coherence and vitality in these individuals [33]. Functional models in rehabilitation nursing emphasize holistic, patient-centered care, guiding nurses and midwives to systematically address complex needs. Integrating brief self-compassion practices within these frameworks can enhance psychological well-being, resilience, and overall adaptation in individuals with physical disabilities [34].
Despite the strengths of the study, several limitations should be acknowledged. First and most critically, the sample size (n = 30) was substantially smaller than the minimum required sample size estimated by our post-hoc power analysis (n = 42 for sleep quality; n = 118 for pain adaptation).
Consequently, the study had insufficient statistical power (0.29 for pain adaptation) to reliably detect the observed medium effect size on pain adaptation, rendering the non-significant finding for this outcome inconclusive. Second, the lack of true randomization limits causal inferences. Third, the study relied exclusively on self-report measures. Fourth, the intervention period was relatively short (8 weeks).
Fifth, the findings may have limited generalizability due to the specific characteristics of the sample. Finally, the absence of a follow-up assessment means the sustainability of improvements could not be evaluated.
Conclusion
The present study provides preliminary evidence that an online mindful self-compassion intervention can significantly improve sleep quality in employees with physical disabilities. However, regarding pain adaptation, the findings are inconclusive due to insufficient statistical power, and no meaningful conclusion can be drawn.
The study should be viewed as a hypothesis-generating investigation rather than a confirmatory trial. Future adequately powered randomized controlled trials are needed. Due to the quasi-experimental design, causal conclusions should be drawn cautiously.
Ethics Consideration
The protocol of this study was approved by the Iran National Committee for Ethics in Biomedical Research (https://ethics.research.ac.ir/IndexEn.php) with code: IR.IAU.SRB.REC.1404.137. This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. Informed consent was obtained from all participants prior to data collection, and participation was voluntary with the right to withdraw at any time. Participant confidentiality and data anonymity were strictly maintained throughout the study.
Acknowledgements
The authors would like to appreciate the participants who cooperated closely with them. In addition, we would like to express our gratitude to the managers and staff of the National Iranian Gas Company.
Conflict of Interest
The authors declared no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors' Contributions
Khodabakhshi-Koolaee A, Shahendeh-Hellabad T, and Falsafinejad MR; Conducting research, data gathering and analysis; Khodabakhshi-Koolaee A, Shahendeh-Hellabad T. Conceptualization: Khodabakhshi-Koolaee A and Falsafinejad MR, study design, and drafting of the initial version; Final approval: All authors.
Artificial Intelligence Utilization
The authors utilized AI to assist with English language editing and ensure compliance with journal standards.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
The present study examined the effectiveness of an online Mindful Self-Compassion program on sleep quality and pain adaptation among physically disabled employees of the National Iranian Gas Company. Individuals with physical disabilities often experience complex challenges such as chronic pain, sleep disturbances, and reduced quality of life, which negatively impact mental health, social functioning, and occupational performance. Addressing these issues through psychological interventions that foster emotional resilience, self-regulation, and self-compassion have become increasingly important.
Effect of the Intervention on Sleep Quality
The results indicated that participation in the Mindful Self-Compassion intervention led to significant improvements in sleep quality, including fewer nocturnal awakenings, reduced sleep difficulties, and greater overall sleep satisfaction. These outcomes align with prior research demonstrating that self-compassion exercises reduce rumination, anxiety, and depression, thereby enhancing overall mental health and well-being.
In line with these findings, it can be argued that the core of compassion-focused therapy lies in self-compassion, care, understanding, and empathy. For a patient, self-compassion involves adopting a positive attitude toward one's current condition, particularly in the presence of uncontrollable chronic illness [23]. One study demonstrated that mindful compassion reduces pain catastrophizing and lowers rumination levels among women with mobility impairments [24]. Other studies have demonstrated, based on the self-regulation behavior model, that self-compassion can promote healthy behaviors, such as sleep, by fostering adaptive emotional states [25]. Specifically, self-compassion has the potential to act as a protective factor for emotional regulation and coping capacities, thereby safeguarding sleep quality [26]. Previous studies have also shown that positive thoughts and self-kindness are adaptive emotions that enhance healthy behaviors and protect sleep quality [25]. Findings suggest that individuals exhibiting higher levels of self-compassion are more likely to adopt positive coping strategies in response to stress [27], potentially because they are more attentive and responsive to their own emotions and needs [26].
Mindfulness plays a key role in this process by cultivating present-moment, nonjudgmental awareness of negative thoughts and emotions, thereby reducing pre-sleep activation of the nervous system. This mechanism is particularly important for individuals with physical disabilities who face stress, worry, and feelings of inefficacy, as it can help increase pre-sleep relaxation and overall sleep quality [14-16]. Research has shown that increasing self-compassion facilitates the mental pathway to sleep by enhancing internal security and reducing self-criticism. Hence, delivering this intervention online not only provides easier accessibility and cost-effectiveness but can also effectively improve sleep quality in individuals with disabilities, ultimately contributing to the psychological and physical well-being of these individuals [17,24].
Effect of the Intervention on Pain Adaptation
In contrast to the findings for sleep quality, no statistically significant effect was observed on adaptation to chronic pain (F = 2.13, p = .151, η² = 0.079). However, this finding must be interpreted very carefully. The observed effect size for pain adaptation was medium (η² = 0.079), but the statistical power was only 0.29, which is far below the recommended minimum of 0.80. This means that even if the intervention had a true medium-sized effect on pain adaptation in the population, this study had only a 29% chance of detecting it as statistically significant. Therefore, the non-significant result is highly likely to be a false negative (Type II error) and should not be taken as evidence that the intervention is ineffective for pain adaptation [29].
The most parsimonious conclusion is that the present study was severely underpowered for this outcome, rendering the p-value uninformative. Post-hoc power analysis indicated that a sample of 118 participants would be required to reliably detect the observed medium effect size. Future studies with adequate sample sizes (approximately 118 participants) are necessary to determine whether online mindful self-compassion therapy truly has no effect on pain adaptation or whether the effect could not be detected here due to insufficient statistical power [18].
Several factors could be considered for future research, but should not be overinterpreted given the primary limitation of low power. First, the Adaptation to Chronic Pain Questionnaire (ACPQ) may lack sensitivity to detect subtle changes in cognitive or emotional coping mechanisms over a short period. Second, the 8-week intervention duration may have been insufficient to modify deeply ingrained cognitions and emotional responses related to chronic pain. Third, the session content, while focused on general mindfulness and self-compassion, may not have been specifically tailored to target pain-related beliefs, coping strategies, or functional adaptation.
Consistent with the need for caution in interpreting null findings, previous studies that reported significant effects of compassion-focused therapy on pain-related outcomes typically had larger sample sizes and longer intervention durations. Psychologically, it shifts individuals' mindset from a "doing mode" to a "being mode" (28). However, these effects may require longer training periods or more pain-specific content than the present 8-week general mindful self-compassion program provided. For example, Mohamadpour [23] demonstrated that compassion-based therapy reduced pain catastrophizing in patients with multiple sclerosis, while Lanzaro et al [29] in their systematic review concluded that studies with sample sizes below 50 participants were consistently underpowered to detect effects on chronic pain outcomes. Similarly, Dou et al [30] found that mindfulness-based interventions required minimum sample sizes of 40–60 participants to detect significant effects on psychological outcomes in clinical populations.
Physiological studies have demonstrated that mindfulness training can reduce pain by altering anterior cingulate and insular cortex activity, alleviate emotional exhaustion, and reduce occupational burnout among nurses [30].
Consistent with the findings of this study, research has shown that compassion-focused therapy, originally developed to reduce high levels of shame and self-criticism, is grounded in evolutionary, social, and neurobiological understandings of human emotions [31]. Compassion-focused therapy aims to activate the soothing and affiliative emotion-regulation system, which is often underdeveloped in individuals with a history of trauma or chronic psychological pain. Integrating compassion-focused therapy with mindfulness, by cultivating self-kindness, emotional courage, and the capacity for compassionate engagement with suffering, further enriches the therapeutic approach [22,32]. Patients with spinal cord injury often struggle with identity disruption, loss of bodily control, and existential fears. Accordingly, Mindful Self-Compassion therapy provides a synergistic framework for restoring psychological coherence and vitality in these individuals [33]. Functional models in rehabilitation nursing emphasize holistic, patient-centered care, guiding nurses and midwives to systematically address complex needs. Integrating brief self-compassion practices within these frameworks can enhance psychological well-being, resilience, and overall adaptation in individuals with physical disabilities [34].
Despite the strengths of the study, several limitations should be acknowledged. First and most critically, the sample size (n = 30) was substantially smaller than the minimum required sample size estimated by our post-hoc power analysis (n = 42 for sleep quality; n = 118 for pain adaptation).
Consequently, the study had insufficient statistical power (0.29 for pain adaptation) to reliably detect the observed medium effect size on pain adaptation, rendering the non-significant finding for this outcome inconclusive. Second, the lack of true randomization limits causal inferences. Third, the study relied exclusively on self-report measures. Fourth, the intervention period was relatively short (8 weeks).
Fifth, the findings may have limited generalizability due to the specific characteristics of the sample. Finally, the absence of a follow-up assessment means the sustainability of improvements could not be evaluated.
Conclusion
The present study provides preliminary evidence that an online mindful self-compassion intervention can significantly improve sleep quality in employees with physical disabilities. However, regarding pain adaptation, the findings are inconclusive due to insufficient statistical power, and no meaningful conclusion can be drawn.
The study should be viewed as a hypothesis-generating investigation rather than a confirmatory trial. Future adequately powered randomized controlled trials are needed. Due to the quasi-experimental design, causal conclusions should be drawn cautiously.
Ethics Consideration
The protocol of this study was approved by the Iran National Committee for Ethics in Biomedical Research (https://ethics.research.ac.ir/IndexEn.php) with code: IR.IAU.SRB.REC.1404.137. This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. Informed consent was obtained from all participants prior to data collection, and participation was voluntary with the right to withdraw at any time. Participant confidentiality and data anonymity were strictly maintained throughout the study.
Acknowledgements
The authors would like to appreciate the participants who cooperated closely with them. In addition, we would like to express our gratitude to the managers and staff of the National Iranian Gas Company.
Conflict of Interest
The authors declared no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors' Contributions
Khodabakhshi-Koolaee A, Shahendeh-Hellabad T, and Falsafinejad MR; Conducting research, data gathering and analysis; Khodabakhshi-Koolaee A, Shahendeh-Hellabad T. Conceptualization: Khodabakhshi-Koolaee A and Falsafinejad MR, study design, and drafting of the initial version; Final approval: All authors.
Artificial Intelligence Utilization
The authors utilized AI to assist with English language editing and ensure compliance with journal standards.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Type of Study: Orginal research |
Subject:
other
References
1. Fakhri M, Khodabakhshi-Koolaee A, Falsafinejad MR. Investigating the predictive role of mental toughness in resilience and distress tolerance of paralympic athletes. Iranian Rehabilitation Journal. 2024;22(3):375-382. [https://doi.org/10.32598/irj.22.3.18.7]
2. Van Dam K, Gielissen M, Bles R, van der Poel A, Boon B. The impact of assistive living technology on perceived independence of people with a physical disability in executing daily activities: a systematic literature review. Disability and Rehabilitation: Assistive Technology. 2024;19(4):1262-1271. [https://doi.org/10.1080/17483107.2022.2162614] [PMID]
3. Oh J, Aquino M. Enhancing health-related fitness, self-efficacy, and quality of life in adults with physical disabilities: a 9-week community-based structured exercise and mindfulness program. Advanced Exercise and Health Science. 2024;1(3):187-194. [https://doi.org/10.1016/j.aehs.2024.07.001]
4. Van Leeuwen CM, Post MW, Van Der Woude LH, De Groot S, Smit C, Van Kuppevelt D, Lindeman E. Changes in life satisfaction in persons with spinal cord injury during and after inpatient rehabilitation: adaptation or measurement bias? Quality of Life Research. 2012;21(9):1499-1508. [https://doi.org/10.1007/s11136-011-0073-7] [PMID]
5. Hammad MA, Alyami MHF, Awed HS. The association between internet addiction and sleep quality among medical students in Saudi Arabia. Annals of Medicine. 2024;56(1):1-8; 2307502. [https://doi.org/10.1080/07853890.2024.2307502] [PMID]
6. Cao Y, Wu H, Shi S, Xie D. Effects of mindfulness-based stress reduction therapy for sleep quality and perceived stress in patients with spinal cord injury. Explore. 2024;20(5):103037. [https://doi.org/10.1016/j.explore.2024.103037] [PMID]
7. Huang S, Lu Z, Xie S, He J, Lu Y, Pang M, Liu B. Low back pain in aging populations: a global analysis of disability and healthcare burden over three decades. Journal of Back and Musculoskeletal Rehabilitation. 2025;39(1):347-356. [https://doi.org/10.1177/10538127251369280] [PMID]
8. Tran J, Dorstyn DS, Burke ALJ. Psychosocial aspects of spinal cord injury pain: a meta-analysis. Spinal Cord. 2016;54(9):640-648. [https://doi.org/10.1038/sc.2016.66] [PMID]
9. Hearn JH, Cross A. Mindfulness for pain, depression, anxiety, and quality of life in people with spinal cord injury: a systematic review. BMC Neurology. 2020;20(1):1-11. [https://doi.org/10.1186/s12883-020-1619-5] [PMID]
10. Gilbert P. The origins and nature of compassion-focused therapy. British Journal of Clinical Psychology. 2014;53(1):6-41. [https://doi.org/10.1111/bjc.12043] [PMID]
11. Gilbert P, Irons C. Compassion focused therapy. In: The Beginner's Guide to Counselling & Psychotherapy. 2015. p. 127. [https://doi.org/10.4135/9781473918061.n11]
12. Neff KD. The role of self-compassion in development: a healthier way to relate to oneself. Human Development. 2009;52(4):211-214. [https://doi.org/10.1159/000215071] [PMID]
13. Terry ML, Leary MR. Self-compassion, self-regulation, and health. Self and Identity. 2011;10(3):352-362. [https://doi.org/10.1080/15298868.2011.558404]
14. Gilbert P. Introducing compassion-focused therapy. Advances in Psychiatric Treatment. 2009;15(3):199-208. [https://doi.org/10.1192/apt.bp.107.005264]
15. Gilbert P, Choden. Mindful compassion. London: Robinson; 2013.
16. Kabat-Zinn J. Mindfulness. Mindfulness. 2015;6(6):1481-1483. [https://doi.org/10.1007/s12671-015-0456-x]
17. Khodabakhshi-Koolaee, A., Ghadyani, S., & Malekitabar, A. Mindfulness-based stress reduction (MBSR) for improving hope and happiness in men with visual impairment. British Journal of Visual Impairment,2026; 44(1): 3-13; [https://doi.org/10.1177/02646196241294212]
18. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods. 2007;39(2):175-191. [https://doi.org/10.3758/BF03193146] [PMID]
19. Buysse DJ, Reynolds III CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Research. 1989;28(2):193-213. [https://doi.org/10.1016/0165-1781(89)90047-4] [PMID]
20. Farrahi Moghaddam J, Nakhaee N, Sheibani V, Garrusi B, Amirkafi A. Reliability and validity of the Persian version of the Pittsburgh Sleep Quality Index (PSQI-P). Sleep and Breathing. 2012;16(1):79-82. [https://doi.org/10.1007/s11325-010-0478-5] [PMID]
21. Zavadilová R, Knotek P. Dotazník adaptace na chronickou bolest. Bolest. 2006; 9:28-33.
22. Hosseininia N, Dousti P, Piryaei N. Psychometric characteristics of the adaptation to chronic pain questionnaire. Recent Innovations in Psychology. 2024;1(3):47-59. [https://doi.org/10.22034/rip.2024.451529.1019]
23. Mohamadpour F. Effectiveness of compassion-based online therapy on suicidal thoughts and pain catastrophizing in female patients with multiple sclerosis in the relapsing-remitting phase. Frontiers in Psychology. 2023; 14: 1-10. [https://doi.org/10.3389/fpsyg.2023.1128308] [PMID]
24. Nooshazari S, Khodabakhshi-Koolaee A, Falsafinejad MR. Efficacy of a mindful compassion intervention on reducing pain catastrophizing and rumination in women with mobility disability: a randomized controlled trial. Preventive Care in Nursing and Midwifery Journal. 2025;15(2):3-12. [https://doi.org/10.61882/pcnm.15.2.3]
25. Sirois FM, Kitner R, Hirsch JK. Self-compassion, affect, and health-promoting behaviors. Health Psychology. 2015;34(6):661-669. [https://doi.org/10.1037/hea0000158] [PMID]
26. Wang Y, Fu T, Wang J, Chen S, Sun G. The relationship between self-compassion, coping style, sleep quality, and depression among college students. Frontiers in Psychology. 2024; 15:1-8. [https://doi.org/10.3389/fpsyg.2024.1378181] [PMID]
27. Ewert C, Vater A, Schroder-Abe M. Self-compassion and coping: a meta-analysis. Mindfulness. 2021;12(5):1063-1077. [https://doi.org/10.1007/s12671-020-01563-8]
28. Li A, Wang S, Cai M, Sun R, Liu X. Self-compassion and life-satisfaction among Chinese self-quarantined residents during the COVID-19 pandemic: a moderated mediation model of positive coping and gender. Personality and Individual Differences. 2021; 170:1-8. [https://doi.org/10.1016/j.paid.2020.110457] [PMID]
29. Lanzaro C, Carvalho SA, Lapa TA, Valentim A, Gago B. A systematic review of self-compassion in chronic pain: from correlation to efficacy. Spanish Journal of Psychology. 2021;24: e26. 1-19. [https://doi.org/10.1017/SJP.2021.22] [PMID]
30. Dou J, Lian Y, Lin L, Asmuri SN, Wang P, Rajen Durai RA. Effectiveness of mindfulness-based interventions on burnout, resilience and sleep quality among nurses: a systematic review and meta-analysis of randomized controlled trials. BMC Nursing. 2025;24(1): 1-14. [https://doi.org/10.1186/s12912-025-03101-0] [PMID]
31. Tahmasebi M, Hossein Fallah M, Yazdi SV. Effectiveness of compassion-focused acceptance and commitment therapy (ACT) on quality of life in male patients with painful spinal cord injury. Mental Health and Lifestyle Journal. 2025;3(1):1-2. [https://doi.org/10.61838/mhlj.3.1.10]
32. Azimi M, Falsafinejad MR, Khodabakhshi-Koolaee A, Jouybari LM. The effect of mindful yoga on fatigue in women with breast cancer: a quasi-experimental study. Jundishapur Journal of Chronic Disease Care. 2025; 14 (14): 1-9. [https://doi.org/10.5812/jjcdc-151438]
33. Jin X, Li H, Chong YY, Mann KF, Yao W, Wong CL. Feasibility and preliminary effects of acceptance and commitment therapy on reducing psychological distress and improving the quality of life of the parents of children with cancer: a pilot randomized controlled trial. Psycho-Oncology. 2023;32(1):165-169. [https://doi.org/10.1002/pon.5941] [PMID]
34. Shirozhan S, Shoja M, Metanat F, Motie M. Functional models in rehabilitation nursing care: a scoping review. Preventive Care in Nursing and Midwifery Journal. 2025;15(3):61-70. [https://doi.org/10.61882/pcnm.15.3.61]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |