
Preventive Care in Nursing and Midwifery Journal

Volume 16, Issue 2 (4-2026)
Prev Care Nurs Midwifery J 2026, 16(2): 29-34 |
Back to browse issues page

Ethics code: 1404.331.IR.GOUMS.REC
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
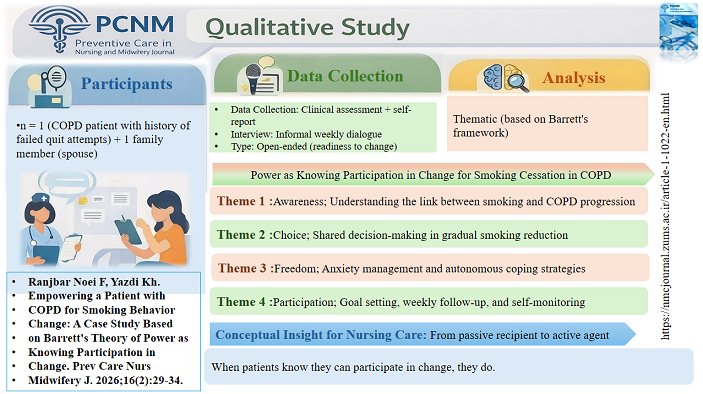
Ranjbar Noei F, Yazdi K. Empowering a Patient with COPD for Smoking Behavior Change: A Case Study Based on Barrett's Theory of Power as Knowing Participation in Change. Prev Care Nurs Midwifery J 2026; 16 (2) :29-34
URL: http://nmcjournal.zums.ac.ir/article-1-1022-en.html
URL: http://nmcjournal.zums.ac.ir/article-1-1022-en.html



School of Nursing and Midwifery, Nursing Research Center, Golestan University of Medical Sciences, Gorgan, Iran , yazdi@goums.ac.ir
Full-Text [PDF 683 kb]
(169 Downloads)
| Abstract (HTML) (244 Views)
Outcome Measures and Data Collection Tools
Data were collected using the following instruments:
A 0–10 numeric rating scale for dyspnea severity
Daily cigarette consumption record sheet
Spirometry testing for pulmonary function (FEV₁)
Assessments were performed at baseline and at the end of the six-month intervention period.
Ethical Considerations
Written informed consent was obtained from the patient prior to participation. Confidentiality and anonymity were strictly maintained throughout the study.
The intervention was implemented as part of nursing care, and institutional ethical approval was obtained from the relevant committee.
Discussion
According to Barrett's theory of power as conscious participation in change [15] our nursing interventions helped the patient overcome the challenges of COPD and smoking cessation through a sequential but non-linear process. First, increasing the patient's awareness of the association between smoking and exacerbation of COPD symptoms (dyspnea 9/10) strengthened his motivation to change behavior by creating cognitive dissonance. Second, offering conscious choice allowed him to select assistive methods aligned with his preferences (e.g., nicotine gum vs. gradual reduction), which enhanced perceived control and intrinsic motivation. Third, the freedom dimension removed perceived external pressure, reducing psychological resistance commonly seen in smokers with prior failed attempts. Fourth, the patient's active participation in designing a smoking cessation program and recording progress transformed him from a passive recipient to an active agent, giving him a sense of control over the treatment process. Finally, the helicy principle reframed setbacks as irreversible forward movement rather than regression, which prevented demoralization when cravings occurred. These mechanisms directly targeted the patient's previous failed attempts, rooted in psychological dependence and anxiety rather than lack of knowledge alone. he results of this study are consistent with previous research on the application of Barrett’s theory in the management of chronic diseases. The Etheridge-Bagley study showed that increasing patients' awareness through this theory improves their participation in the change process [12]. Chang's study also confirmed the positive impact of individual empowerment-based interventions on patients' quality of life. However, the main difference of this study was the practical application of Barrett’s theory in smoking cessation in COPD patients, which has received less attention in the literature [14]. Dehkordi's study also emphasized the importance of self-management in COPD but used traditional self-care models. While the present study, by integrating Barrett’s theory, emphasized the role of patient agency [2]. Andy's study, which was conducted as a systematic review, also showed that behavioral interventions such as gradual smoking reduction are effective in smoking cessation, but the present study examined the patient's lived experience with a qualitative approach [8]. Also, unlike studies such as Hübsch that focused on post-discharge interventions, this study used Barrett’s theory to empower patients during hospitalization [6]. While studies such as Siltanen emphasized the role of the family in self-management, this study demonstrated how active patient participation (alone) can facilitate behavior change [1].
The innovation of the present study is the combination of Barrett’s theory with standard smoking cessation interventions (such as gradual reduction in consumption and psychological support) and patient participation in decision-making, which is in line with the principles of individualized care in modern nursing.
This study has several limitations. As a single-case design, the findings cannot be generalized to broader populations. The absence of a control group limits causal inference, and smoking reduction was self-reported, which may introduce reporting bias. The follow-up period of six months may also be insufficient to assess long-term abstinence.
Despite these limitations, a key strength of this study is the theory-driven, individualized intervention grounded in Barrett’s framework, which addresses both psychological and behavioral aspects of smoking dependence. The integration of empowerment strategies within routine hospital care is another notable strength.
Future research should include randomized controlled trials with larger samples and longer follow-up periods (≥12 months). Biochemical validation of smoking status (e.g., exhaled carbon monoxide) is also recommended. Comparative studies between Barrett’s theory and other behavioral models may further clarify its relative effectiveness in smoking cessation interventions.
Conclusion
This case illustrates that Barrett’s theory can serve as an effective framework for supporting smoking cessation in COPD patients with a history of failed quit attempts. The findings suggest that enhancing awareness, offering meaningful choices, supporting autonomy, and promoting active participation can facilitate sustained behavioral change beyond traditional educational approaches. The helicy principle is particularly valuable in reframing relapse as part of a continuous, non-linear process, thereby maintaining patient motivation.
For clinical practice, nurses can apply this framework to structure brief, patient-centered interventions during hospitalization. Even short empowerment-focused interactions may initiate meaningful behavioral change in high-risk COPD patients and support long-term self-management.
Ethics Consideration
The study was approved by the Research Council and the Biomedical Ethics Committee of Golestan University of Medical Sciences (IR.GOUMS.REC.1404.331). Written informed consent was obtained from the patient before participation and publication of this case report, in accordance with the Declaration of Helsinki.
Acknowledgements
We would like to thank the patient and his wife who participated in this study.
Conflict of Interest
This study has no conflicts of interest.
Funding
Self-funded.
Authors' Contributions
Ranjbar Noei; F: Conceptualization, Investigation (intervention implementation & data collection), Formal Analysis (qualitative interpretation of findings), Writing – original draft.
Yazdi; Kh: Methodology, Validation (verification of data interpretation), Supervision, Writing – review & editing.
Artificial Intelligence Utilization
Not used.
Data Availability Statement
It will remain confidential to the first author.
Full-Text: (56 Views)
Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive, lifelong disease [1]. The global prevalence is increasing (12% worldwide and 4.9% in Iran), mainly due to tobacco use and air pollution [2, 3]. Acute exacerbations are a common complication of the disease, leading to increased hospitalization, costs, and mortality [4, 5]. Behavioral interventions such as early detection, symptom management, smoking cessation, vaccination, and dyspnea management can help reduce exacerbations and hospitalizations [6]. Smoking is the primary cause of COPD and has systemic effects [7]. Although behavioral therapies are effective in smoking cessation [8]. However, their implementation in hospital settings is often limited by prioritization of acute conditions, lack of resources and expertise, and inadequate financial reimbursement [9, 10].
In this context, nursing models based on theoretical frameworks can provide valuable guidance for improving care, promoting health, and supporting patient recovery [11].
Barrett’s Theory of Power as Knowing Participation in Change emphasizes awareness, choice, intentional action, and participation in change processes [12]. The theory does not prescribe a fixed order for these concepts, as their importance may vary across contexts [13]. The theory suggests that nurses should be aware of their choices and feel free to initiate change across different domains [14]. Barrett distinguishes between power-as-control (hierarchical and deterministic) and power-as-freedom (relational and participatory). Without awareness, meaningful change is unlikely; individuals must actively participate in creating new realities and use power as a resource for achieving health-related goals [13].
Objectives
The aim of this case study was to explore changes in smoking behavior and patient empowerment following a nursing intervention based on Barrett’s Theory of Power as Knowing Participation in Change in a patient with COPD and previous unsuccessful smoking cessation attempts.
Barrett's Theory as Knowing Model
The Theory of Power as Knowing Participation in Change, developed by Barrett from Rogers’ Science of Unitary Human Beings, defines power as the capacity to consciously participate in change through four dimensions: awareness, choice, intentional action, and participation [13]. The theory was operationalized in nursing practice through the Health Patterning Model, which focuses on enhancing patient awareness and agency during the change process [15]. Rogers’ concepts of resonancy and helicy describe change as continuous and nonlinear, emphasizing that human processes evolve in a dynamic and irreversible way [16,17]. Barrett also distinguishes between power-as-control and power-as-freedom, highlighting the role of autonomy and participation in facilitating meaningful change [13]. In this study, the theory was used to support smoking behavior change by increasing awareness of smoking risks, promoting autonomous decision-making, and encouraging active participation in care planning. Interventions included pattern recognition, exploration of patient experiences, identification of barriers, goal setting, and progress monitoring [15]. Barrett’s theory was selected due to its emphasis on autonomy rather than authority, its relevance to psychological dependence in COPD-related smoking behavior, and its alignment with the nonlinear nature of behavioral change in chronic illness.
Methods
Study Design
This is a single-case study conducted according to the CARE reporting guidelines.
Study Setting
The study was conducted in a teaching hospital affiliated with Golestan University of Medical Sciences in northern Iran.
Patient Information
A 55-year-old male construction worker with a diploma-level education was admitted with a diagnosis of chronic obstructive pulmonary disease (COPD). He had a 30-year history of smoking approximately one pack of cigarettes per day and reported multiple unsuccessful attempts to quit smoking. The patient experienced progressive dyspnea, chronic cough with sputum production, wheezing, and reduced physical activity tolerance. He also reported psychological dependence on smoking. His spouse provided emotional support during hospitalization. The patient was purposively selected due to recurrent COPD-related hospital admissions and a history of failed smoking cessation attempts. The patient and nurse jointly agreed on the intervention goals at baseline, in accordance with Barrett’s participatory approach (Table 1).
Chronic obstructive pulmonary disease (COPD) is a progressive, lifelong disease [1]. The global prevalence is increasing (12% worldwide and 4.9% in Iran), mainly due to tobacco use and air pollution [2, 3]. Acute exacerbations are a common complication of the disease, leading to increased hospitalization, costs, and mortality [4, 5]. Behavioral interventions such as early detection, symptom management, smoking cessation, vaccination, and dyspnea management can help reduce exacerbations and hospitalizations [6]. Smoking is the primary cause of COPD and has systemic effects [7]. Although behavioral therapies are effective in smoking cessation [8]. However, their implementation in hospital settings is often limited by prioritization of acute conditions, lack of resources and expertise, and inadequate financial reimbursement [9, 10].
In this context, nursing models based on theoretical frameworks can provide valuable guidance for improving care, promoting health, and supporting patient recovery [11].
Barrett’s Theory of Power as Knowing Participation in Change emphasizes awareness, choice, intentional action, and participation in change processes [12]. The theory does not prescribe a fixed order for these concepts, as their importance may vary across contexts [13]. The theory suggests that nurses should be aware of their choices and feel free to initiate change across different domains [14]. Barrett distinguishes between power-as-control (hierarchical and deterministic) and power-as-freedom (relational and participatory). Without awareness, meaningful change is unlikely; individuals must actively participate in creating new realities and use power as a resource for achieving health-related goals [13].
Objectives
The aim of this case study was to explore changes in smoking behavior and patient empowerment following a nursing intervention based on Barrett’s Theory of Power as Knowing Participation in Change in a patient with COPD and previous unsuccessful smoking cessation attempts.
Barrett's Theory as Knowing Model
The Theory of Power as Knowing Participation in Change, developed by Barrett from Rogers’ Science of Unitary Human Beings, defines power as the capacity to consciously participate in change through four dimensions: awareness, choice, intentional action, and participation [13]. The theory was operationalized in nursing practice through the Health Patterning Model, which focuses on enhancing patient awareness and agency during the change process [15]. Rogers’ concepts of resonancy and helicy describe change as continuous and nonlinear, emphasizing that human processes evolve in a dynamic and irreversible way [16,17]. Barrett also distinguishes between power-as-control and power-as-freedom, highlighting the role of autonomy and participation in facilitating meaningful change [13]. In this study, the theory was used to support smoking behavior change by increasing awareness of smoking risks, promoting autonomous decision-making, and encouraging active participation in care planning. Interventions included pattern recognition, exploration of patient experiences, identification of barriers, goal setting, and progress monitoring [15]. Barrett’s theory was selected due to its emphasis on autonomy rather than authority, its relevance to psychological dependence in COPD-related smoking behavior, and its alignment with the nonlinear nature of behavioral change in chronic illness.
Methods
Study Design
This is a single-case study conducted according to the CARE reporting guidelines.
Study Setting
The study was conducted in a teaching hospital affiliated with Golestan University of Medical Sciences in northern Iran.
Patient Information
A 55-year-old male construction worker with a diploma-level education was admitted with a diagnosis of chronic obstructive pulmonary disease (COPD). He had a 30-year history of smoking approximately one pack of cigarettes per day and reported multiple unsuccessful attempts to quit smoking. The patient experienced progressive dyspnea, chronic cough with sputum production, wheezing, and reduced physical activity tolerance. He also reported psychological dependence on smoking. His spouse provided emotional support during hospitalization. The patient was purposively selected due to recurrent COPD-related hospital admissions and a history of failed smoking cessation attempts. The patient and nurse jointly agreed on the intervention goals at baseline, in accordance with Barrett’s participatory approach (Table 1).
| Participant | Goals |
| Patient | To quit smoking and improve respiratory status. |
| Nurse | To support smoking cessation, improve breathing, and enhance quality of life. |
Clinical findings at Baseline
At admission, the patient’s dyspnea severity was rated 9/10 on a numeric rating scale. Vital signs included respiratory rate 23 breaths/min, heart rate 83 beats/min, blood pressure 110/83 mmHg, temperature 36.7°C, and oxygen saturation 88%. Spirometry results confirmed moderate COPD with a forced expiratory volume in one second (FEV₁) of 60% predicted, consistent with GOLD stage II classification.
Timeline of Intervention
The intervention was implemented over a six-month period. Baseline assessment was conducted at admission, followed by initiation of the nursing intervention. Weekly structured follow-up sessions were conducted during hospitalization and after discharge through outpatient visits and telephone follow-ups.
Final evaluation of outcomes was performed at the end of the six-month period.
Nursing Intervention Based on Barrett’s Theory
A structured nursing intervention grounded in Barrett’s Theory of Power as Knowing Participation in Change was applied to support smoking behavior change and patient empowerment. The intervention was designed according to four core dimensions of the theory:
Awareness: Education was provided regarding the relationship between smoking and COPD progression, along with training in breathing techniques and symptom awareness.
Choice: The patient was actively involved in shared decision-making to develop a gradual smoking reduction plan based on his readiness to change.
Intentional action (freedom): Anxiety management strategies, coping skills, and individualized respiratory care techniques were introduced to enhance autonomy and self-regulation.
Participation: The patient engaged in goal setting, care planning, and weekly monitoring of progress throughout the intervention period.
The intervention also included psychosocial support and family involvement. Each session lasted approximately 30–45 minutes and was delivered on a weekly basis by the nursing researcher.
Other components of Barrett’s framework such as guided imagery, therapeutic touch, dream analysis, meditation, and administration of the PKPCT questionnaire were not included in this intervention. The full nursing process is presented in Table 2.
Nursing Diagnoses
Based on the North American Nursing Diagnosis Association (NANDA-I) classification system, the following nursing diagnoses were identified:
At admission, the patient’s dyspnea severity was rated 9/10 on a numeric rating scale. Vital signs included respiratory rate 23 breaths/min, heart rate 83 beats/min, blood pressure 110/83 mmHg, temperature 36.7°C, and oxygen saturation 88%. Spirometry results confirmed moderate COPD with a forced expiratory volume in one second (FEV₁) of 60% predicted, consistent with GOLD stage II classification.
Timeline of Intervention
The intervention was implemented over a six-month period. Baseline assessment was conducted at admission, followed by initiation of the nursing intervention. Weekly structured follow-up sessions were conducted during hospitalization and after discharge through outpatient visits and telephone follow-ups.
Final evaluation of outcomes was performed at the end of the six-month period.
Nursing Intervention Based on Barrett’s Theory
A structured nursing intervention grounded in Barrett’s Theory of Power as Knowing Participation in Change was applied to support smoking behavior change and patient empowerment. The intervention was designed according to four core dimensions of the theory:
Awareness: Education was provided regarding the relationship between smoking and COPD progression, along with training in breathing techniques and symptom awareness.
Choice: The patient was actively involved in shared decision-making to develop a gradual smoking reduction plan based on his readiness to change.
Intentional action (freedom): Anxiety management strategies, coping skills, and individualized respiratory care techniques were introduced to enhance autonomy and self-regulation.
Participation: The patient engaged in goal setting, care planning, and weekly monitoring of progress throughout the intervention period.
The intervention also included psychosocial support and family involvement. Each session lasted approximately 30–45 minutes and was delivered on a weekly basis by the nursing researcher.
Other components of Barrett’s framework such as guided imagery, therapeutic touch, dream analysis, meditation, and administration of the PKPCT questionnaire were not included in this intervention. The full nursing process is presented in Table 2.
Nursing Diagnoses
Based on the North American Nursing Diagnosis Association (NANDA-I) classification system, the following nursing diagnoses were identified:
- Ineffective breathing pattern.
- Impaired gas exchange.
- Ineffective health maintenance related to smoking dependence.
- Anxiety related to dyspnea and chronic illness.
| Nursing Stage | Content |
| Assessment | Data were collected through patient and family interviews, medical records, and clinical examination. Patient perceptions, smoking behavior, respiratory status, and psychosocial factors were assessed. Baseline findings included dyspnea (9/10), FEV₁ 60%, oxygen saturation 88%, and smoking history of 20 cigarettes/day. |
| Nursing Diagnoses (NANDA-I) | Ineffective breathing pattern; impaired gas exchange; ineffective health maintenance; anxiety; fear related to smoking cessation and disease progression. |
| Goals | Reduce dyspnea, decrease smoking behavior, improve respiratory status, reduce anxiety, and enhance patient awareness and empowerment. |
| Planning | Education on smoking risks, breathing exercises, gradual smoking reduction plan, anxiety management, and strengthening social support. |
| Implementation (Barrett-based intervention) | Awareness: education on COPD–smoking link. Choice: shared decision-making for quitting plan. Freedom: patient autonomy in quitting process. Participation: goal setting, weekly follow-up, self-monitoring of smoking. |
| Evaluation | Dyspnea reduced from 9/10 to 5/10; smoking decreased from 20 to 10 cigarettes/day; improved patient engagement and anxiety reduction reported. |
| Key Barriers/Facilitators | Psychological dependence, previous failed quit attempts; facilitators included family support and motivational reinforcement. |
Nursing Diagnoses
Based on the North American Nursing Diagnosis Association (NANDA-I) classification system, the following nursing diagnoses were identified:
Based on the North American Nursing Diagnosis Association (NANDA-I) classification system, the following nursing diagnoses were identified:
- Ineffective breathing pattern.
- Impaired gas exchange.
- Ineffective health maintenance related to smoking dependence.
- Anxiety related to dyspnea and chronic illness.
Outcome Measures and Data Collection Tools
Data were collected using the following instruments:
A 0–10 numeric rating scale for dyspnea severity
Daily cigarette consumption record sheet
Spirometry testing for pulmonary function (FEV₁)
Assessments were performed at baseline and at the end of the six-month intervention period.
Ethical Considerations
Written informed consent was obtained from the patient prior to participation. Confidentiality and anonymity were strictly maintained throughout the study.
The intervention was implemented as part of nursing care, and institutional ethical approval was obtained from the relevant committee.
Discussion
According to Barrett's theory of power as conscious participation in change [15] our nursing interventions helped the patient overcome the challenges of COPD and smoking cessation through a sequential but non-linear process. First, increasing the patient's awareness of the association between smoking and exacerbation of COPD symptoms (dyspnea 9/10) strengthened his motivation to change behavior by creating cognitive dissonance. Second, offering conscious choice allowed him to select assistive methods aligned with his preferences (e.g., nicotine gum vs. gradual reduction), which enhanced perceived control and intrinsic motivation. Third, the freedom dimension removed perceived external pressure, reducing psychological resistance commonly seen in smokers with prior failed attempts. Fourth, the patient's active participation in designing a smoking cessation program and recording progress transformed him from a passive recipient to an active agent, giving him a sense of control over the treatment process. Finally, the helicy principle reframed setbacks as irreversible forward movement rather than regression, which prevented demoralization when cravings occurred. These mechanisms directly targeted the patient's previous failed attempts, rooted in psychological dependence and anxiety rather than lack of knowledge alone. he results of this study are consistent with previous research on the application of Barrett’s theory in the management of chronic diseases. The Etheridge-Bagley study showed that increasing patients' awareness through this theory improves their participation in the change process [12]. Chang's study also confirmed the positive impact of individual empowerment-based interventions on patients' quality of life. However, the main difference of this study was the practical application of Barrett’s theory in smoking cessation in COPD patients, which has received less attention in the literature [14]. Dehkordi's study also emphasized the importance of self-management in COPD but used traditional self-care models. While the present study, by integrating Barrett’s theory, emphasized the role of patient agency [2]. Andy's study, which was conducted as a systematic review, also showed that behavioral interventions such as gradual smoking reduction are effective in smoking cessation, but the present study examined the patient's lived experience with a qualitative approach [8]. Also, unlike studies such as Hübsch that focused on post-discharge interventions, this study used Barrett’s theory to empower patients during hospitalization [6]. While studies such as Siltanen emphasized the role of the family in self-management, this study demonstrated how active patient participation (alone) can facilitate behavior change [1].
The innovation of the present study is the combination of Barrett’s theory with standard smoking cessation interventions (such as gradual reduction in consumption and psychological support) and patient participation in decision-making, which is in line with the principles of individualized care in modern nursing.
This study has several limitations. As a single-case design, the findings cannot be generalized to broader populations. The absence of a control group limits causal inference, and smoking reduction was self-reported, which may introduce reporting bias. The follow-up period of six months may also be insufficient to assess long-term abstinence.
Despite these limitations, a key strength of this study is the theory-driven, individualized intervention grounded in Barrett’s framework, which addresses both psychological and behavioral aspects of smoking dependence. The integration of empowerment strategies within routine hospital care is another notable strength.
Future research should include randomized controlled trials with larger samples and longer follow-up periods (≥12 months). Biochemical validation of smoking status (e.g., exhaled carbon monoxide) is also recommended. Comparative studies between Barrett’s theory and other behavioral models may further clarify its relative effectiveness in smoking cessation interventions.
Conclusion
This case illustrates that Barrett’s theory can serve as an effective framework for supporting smoking cessation in COPD patients with a history of failed quit attempts. The findings suggest that enhancing awareness, offering meaningful choices, supporting autonomy, and promoting active participation can facilitate sustained behavioral change beyond traditional educational approaches. The helicy principle is particularly valuable in reframing relapse as part of a continuous, non-linear process, thereby maintaining patient motivation.
For clinical practice, nurses can apply this framework to structure brief, patient-centered interventions during hospitalization. Even short empowerment-focused interactions may initiate meaningful behavioral change in high-risk COPD patients and support long-term self-management.
Ethics Consideration
The study was approved by the Research Council and the Biomedical Ethics Committee of Golestan University of Medical Sciences (IR.GOUMS.REC.1404.331). Written informed consent was obtained from the patient before participation and publication of this case report, in accordance with the Declaration of Helsinki.
Acknowledgements
We would like to thank the patient and his wife who participated in this study.
Conflict of Interest
This study has no conflicts of interest.
Funding
Self-funded.
Authors' Contributions
Ranjbar Noei; F: Conceptualization, Investigation (intervention implementation & data collection), Formal Analysis (qualitative interpretation of findings), Writing – original draft.
Yazdi; Kh: Methodology, Validation (verification of data interpretation), Supervision, Writing – review & editing.
Artificial Intelligence Utilization
Not used.
Data Availability Statement
It will remain confidential to the first author.
Type of Study: case report |
Subject:
Nursing
References
1. Siltanen H, Jylhä V, Holopainen A, Paavilainen E. Family members' experiences and expectations of self-management counseling while caring for a person with chronic obstructive pulmonary disease: a systematic review of qualitative evidence. JBI Evidence Synthesis. 2019;17(11): 2214-2247. [https://doi.org/10.11124/JBISRIR-D-19-00056] [PMID]
2. Dehkordi AH, Heidari-Beni F, Reiszadeh I, Hosseini M, Ali FK. Effect of self-management program on health status and dyspnea in patients with chronic obstructive pulmonary disease. Tanaffos. 2022;21(1): 96-103. [https://www.tanaffosjournal.ir/article_254233.html]
3. Pradana A, Sari DK, Rusda M, Tarigan AP, Wiyono WH, Soeroso NN, et al. Protective effects of probiotics against systemic inflammation in Mice model with chronic obstructive pulmonary disease induced by cigarette-smoke. Reports of Biochemistry and Molecular Biology. 2024;13(3):322-328. [https://doi.org/10.61186/rbmb.13.3.322] [PMID]
4. Ur Rehman A, Ahmad Hassali MA, Muhammad SA, Shah S, Abbas S, Hyder Ali IAB, Salman A. The economic burden of chronic obstructive pulmonary disease (COPD) in the USA, Europe, and Asia: results from a systematic review of the literature. Expert Review of Pharmacoeconomics & Outcomes Research. 2020;20(6): 661-672. [https://doi.org/10.1080/14737167.2020.1678385] [PMID]
5. Venkatesan P. GOLD COPD report: 2024 update. The Lancet Respiratory Medicine. 2024;12(1): 15-16. [https://doi.org/10.1016/S2213-2600(23)00461-7] [PMID]
6. Hübsch C, Clarenbach CF, Franzen DP, Schmid-Mohler G. Post-acute care interventions in patients hospitalized due to COPD exacerbation before and after implementation of an integrated care program. International Journal of Chronic Obstructive Pulmonary Disease. 2025;20:207-216. [https://doi.org/10.2147/COPD.S496167] [PMID]
7. Fabbri LM. Smoking, not COPD, as the disease. New England Journal of Medicine. 2016;374(19):1885-1886. [https://doi.org/10.1056/NEJMe1515508] [PMID]
8. Andy A. Role of behavioral interventions in smoking cessation: a comprehensive review. Depression.2021;9(4):1-3. [https://scholar.google.com/scholar?q=Andy+A+Role+of+Behavioral+Interventions+in+Smoking+Cessation+20]
9. Calle Rubio M, López-Campos JL, Soler-Cataluña JJ, Alcázar Navarrete B, Soriano JB, Rodríguez González-Moro JM, et al. Variability in adherence to clinical practice guidelines and recommendations in COPD outpatients: a multi-level, cross-sectional analysis of the EPOCONSUL study. Respiratory Research. 2017;18(1):1-14. [https://doi.org/10.1186/s12931-017-0685-8] [PMID]
10. Seys D, Bruyneel L, Decramer M, Lodewijckx C, Panella M, Sermeus W, et al. An international study of adherence to guidelines for patients hospitalised with a COPD exacerbation. COPD: Journal of Chronic Obstructive Pulmonary Disease. 2017;14(2):156-163. [https://doi.org/10.1080/15412555.2016.1257599] [PMID]
11. Montano AR. Neuman systems model with nurse-led interprofessional collaborative practice. Nursing Science Quarterly. 2021;34(1):45-53. [https://doi.org/10.1177/0894318420965219] [PMID]
12. Etheridge-Bagley E. Barrett's power theory: re-conceptualizing the pediatric organ donation experience with letter writing. Nursing Science Quarterly. 2022;35(4):427-432. [https://doi.org/10.1177/08943184221115146] [PMID]
13. Barrett EAM. Barrett's theory of power as knowing participation in change. n: Smith MC, Parker ME, editors. Nursing Theories & Nursing Practice. 4th ed. Philadelphia, PA: F.A. Davis Company; 2015. p. 495-508. ISBN: 9780803633124.
14. Chang SJ, Kwak EY, Hahm BJ, Seo SH, Lee da W, Jang SJ. Effects of a meditation program on nurses' power and quality of life. Nursing Science Quarterly. 2016;29(3): 227-234. [https://doi.org/10.1177/0894318416647778] [PMID]
15. Barrett EAM. Power as knowing participation in change: What's new and what's next. Nursing Science Quarterly. 2010;23(1):47-54. [https://doi.org/10.1177/0894318409353797] [PMID]
16. Matthews E. Power perception and critical thinking promotion of clinical nursing instructors [doctoral dissertation]. Charlottetown, PE, Canada: Faculty of Nursing, University of Prince Edward Island; 2024. islandora.upei.ca
17. Barrett EAM. Caroselli C. Methodological ponderings related to the power as knowing participation in change tool. Nursing Science Quarterly. 1998;11(1):17-22. [https://doi.org/10.1177/089431849801100106] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |